From: Tom Fadial. Seizure. ddxof. 2015. Differential Diagnosis of Seizure (ddxof.com)
Adapted from: Tom Fadial. Seizure. ddxof. 2015. Differential Diagnosis of Seizure (ddxof.com)
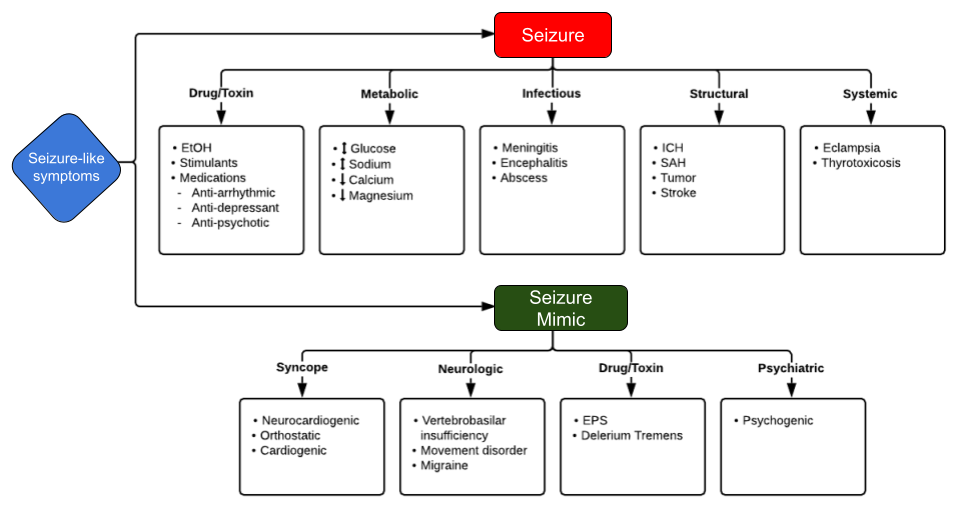
Seizure DDx
Differential diagnosis is broad, but consider these conditions which may mimic epileptic seizures:
References
1. Steven Schater. Differential Diagnosis. Epilepsy Foundation. 2004. Differential Diagnosis | Epilepsy Foundation
2. Tom Fadial. Seizure. ddxof. 2015. Differential Diagnosis of Seizure (ddxof.com)
3. Steven Schater. Wrong Diagnosis. Epilepsy Foundation. 2008. Wrong Diagnosis | Epilepsy Foundation

From: Tom Fadial. Seizure. ddxof. 2015. Differential Diagnosis of Seizure (ddxof.com
This ultrasound shows a normal lung with sliding.
|
Potential Cause |
How to Identify |
Treatments |
|
Hypovolemia |
Rapid heart rate and narrow QRS on ECG; other symptoms of low volume |
Infusion of normal saline or Ringer’s lactate |
|
Hypoxia |
Slow heart rate |
Airway management and effective oxygenation |
|
Hydrogen ion excess (acidosis) |
Low amplitude QRS on the ECG |
Hyperventilation; consider sodium bicarbonate bolus |
|
Hypoglycemia* |
Bedside glucose testing |
IV bolus of dextrose |
|
Hypokalemia |
Flat T waves and appearance of a U wave on the ECG |
IV Magnesium infusion |
|
Hyperkalemia |
Peaked T waves and wide QRS complex on the ECG |
Consider calcium chloride, sodium bicarbonate, and an insulin and glucose protocol |
|
Hypothermia |
Typically preceded by exposure to a cold environment |
Gradual rewarming |
|
Tension pneumothorax |
Slow heart rate and narrow QRS complexes on the ECG; difficulty breathing |
Thoracostomy or needle decompression |
|
Tamponade – Cardiac |
Rapid heart rate and narrow QRS complexes on the ECG |
Pericardiocentesis |
|
Toxins |
Typically will be seen as a prolonged QT interval on the ECG; may see neurological symptoms |
Based on the specific toxin |
|
Thrombosis (pulmonary embolus) |
Rapid heart rate with narrow QRS complexes on the ECG |
Surgical embolectomy or administration of fibrinolytics |
|
Thrombosis (myocardial infarction) |
ECG will be abnormal based on the location of the infarction |
Dependent on extent and age of MI |
*Hypoglycemia is not officially one of the H’s and T’s for adults, but it still can be an important cause of PEA, especially in children. If another reversible cause has not been discovered or if the patient is known to be susceptible to hypoglycemia (e.g., brittle diabetes, past surreptitious use of insulin) then this potential cause of PEA should be considered.
Rapid Sequence Intubation
Rapid Sequence Intubation (RSI) is an airway management technique that creates the optimal conditions for intubation. It induces immediate unresponsiveness through an induction agent and muscular relaxation through a neuromuscular blocking agent1-3. It is generally seen as the fastest and most effective means of controlling the emergency airway.
Indications for Intubation
In this scenario, RSI was indicated by decreased LOC (which increases the risk for airway deterioration) and by the upcoming patient transfer, where it would enhance safety during transport.
Indications and Contraindications for RSI1
|
For
|
Against
|
Administer
Administer RSI: The 9 (or 10) Ps
Planning for RSI - Equipment and Roles
Roles: Should be a minimum of 3 people - Airway proceduralist, Airway assistant, Drug administrator (Team leader can perform one of the above, but ideally should be in a separate standalone role)1
Other Roles: Person to perform MILS if indicated, Person to perform cricoid pressure (if necessary), Scribe1
Preparation requires control over: Self, Patient, Others, Environment
Mnemonics to assist with preparation1
| O2 MARBLES | SOAPME |
|
|
Drugs: Premedication, Induction, Neuromuscular Blockers
Premedication - Note: There is little evidence that these are beneficial clinically, outside of atropine in children.
Induction1
Paralytic Agents1
References
1. Nickson C (2020). Rapid Sequence Intubation (RSI). Life in The Fast Lane. Rapid Sequence Intubation (RSI) • LITFL • CCC Airway
2. Rapid Sequence Intubation (RSI). Westchester Medical Centre Health Network. RSI Information Margaretville only 2.28.17.pdf (hahv.org)
3. Smith C (2001). Rapid Sequence Intubation in Adults: Indications and Concerns. Clinical Pulmonary Medicine. 8(3) pp147-165. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=ovfte&NEWS=N&AN=00045413-200105000-00004.
4. Braude D (2007). Ten Ps of Rapid Sequence Intubation. Emergency Medicine News. 29(1) pp8,12. doi: 10.1097/01.EEM.0000264634.15897.25
5. Szyld D (2010). Paucis Verbis card: Rapid Sequence Intubation. ALiEM. Paucis Verbis card: Rapid Sequence Intubation (aliem.com)
6. Vafier J (2008). Rapid Sequence Intubation. Virginia Department of Health. Microsoft PowerPoint - RSI.ppt (virginia.gov)
|
Acute Respiratory Failure |
|
|
Respiratory Distress: Dyspnea, tachypnea (RR > 20), decreased respirations (RR < 10) or wheezing, labored breathing, nasal flaring, grunting, accessory muscle use, retractions, cyanosis, respiratory arrest |
|
|
Hypoxemic |
Hypercapnic |
|
Known as: Type I ARF, Lung Failure, Oxygenation Failure, Respiratory Insufficiency |
Known as: Type II ARF, Pump Failure, Ventilatory Failure |
|
Definition: The failure of the lungs and heart to provide adequate O2 |
Definition: The failure of the lungs to eliminate adequate CO2 |
|
Criteria: PaO2 < 60mmHg on FiO2 > .50 OR PaO2 < 40mmHg on any FiO2 OR SpO2 < 91% on room air OR P/F ratio (PO2/FiO2)< 300 |
Criteria: paCO2 > 50mmHg w/ pH < 7.35 OR If baseline known, paCO2 = baseline + 10-15mmHg |
References:
1. Pinson & Tang. Acute Respiratory Failure - All there is to Know. Pinson and Tang. September 2017. Acute Respiratory Failure - All There Is To Know | Pinson & Tang (pinsonandtang.com)
|
Potential Cause |
How to Identify |
Treatments |
|
Hypovolemia |
Rapid heart rate and narrow QRS on ECG; other symptoms of low volume |
Infusion of normal saline or Ringer’s lactate |
|
Hypoxia |
Slow heart rate |
Airway management and effective oxygenation |
|
Hydrogen ion excess (acidosis) |
Low amplitude QRS on the ECG |
Hyperventilation; consider sodium bicarbonate bolus |
|
Hypoglycemia* |
Bedside glucose testing |
IV bolus of dextrose |
|
Hypokalemia |
Flat T waves and appearance of a U wave on the ECG |
IV Magnesium infusion |
|
Hyperkalemia |
Peaked T waves and wide QRS complex on the ECG |
Consider calcium chloride, sodium bicarbonate, and an insulin and glucose protocol |
|
Hypothermia |
Typically preceded by exposure to a cold environment |
Gradual rewarming |
|
Tension pneumothorax |
Slow heart rate and narrow QRS complexes on the ECG; difficulty breathing |
Thoracostomy or needle decompression |
|
Tamponade – Cardiac |
Rapid heart rate and narrow QRS complexes on the ECG |
Pericardiocentesis |
|
Toxins |
Typically will be seen as a prolonged QT interval on the ECG; may see neurological symptoms |
Based on the specific toxin |
|
Thrombosis (pulmonary embolus) |
Rapid heart rate with narrow QRS complexes on the ECG |
Surgical embolectomy or administration of fibrinolytics |
|
Thrombosis (myocardial infarction) |
ECG will be abnormal based on the location of the infarction |
Dependent on extent and age of MI |
*Hypoglycemia is not officially one of the H’s and T’s for adults, but it still can be an important cause of PEA, especially in children. If another reversible cause has not been discovered or if the patient is known to be susceptible to hypoglycemia (e.g., brittle diabetes, past surreptitious use of insulin) then this potential cause of PEA should be considered.
Cushing's Triad: Cushing's Triad is a set of three primary signs that often indicate an increased ICP. They are: a change in respirations - often irregular and deep, a widening pulse pressure, and bradycardia.
Clinical Findings Indicating Elevated ICP in Children:
Reference
1. Robert C Tasker. Elevated Intracranial Pressure (ICP) in Children: Clinical Manifestations and Diagnosis. UpToDate. 13 Feb 2020. Elevated intracranial pressure (ICP) in children: Clinical manifestations and diagnosis - UpToDate
EARLY INVOLVEMENT OF A NEUROSURGEON SHOULD OCCUR FOR ALL CHILDREN WITH SIGNS OF INCREASED ICP OR HERNIATION, IF POSSIBLE
| General Measures for Stabilization and Management of Increased ICP |
|
1. Secure the airway with RSI (using C-Spine immobilization in trauma patients) for the following:
Maintain PaCO2 at 35 to 40mmHg in intubated patients, unless signs of herniation |
| 2. Rapid treatment of hypoxia, hypercarbia, hypotension, maintain normal oxygenation |
| 3. Check for, and treat, hypoglycemia + Maintain hemoglobin >70g/L |
| 4. Elevate head 15-30 degrees and keep head midline |
| 5. Aggressively treat fever using antipyretics or cooling blankets |
| 6. Maintain paralysis and control shivering using muscle relaxants (vecuronium, rocuronium) |
| 7. Administer prophylactic anticonvulsants (levetiracetam, phenytoin, phenobarbital) to those who are at high risk of seizure (severe TBI, depressed skull fracture, parenchymal abnormalities) |
| 8. Maintain adequate analgesia (to blunt response to noxious stimuli) and sedation |
|
9. For Intubated Patients:
|
References
1. Robert Tasker. Elevated Intracranial Pressure (ICP) in Children: Management. UpToDate. 4 January 2021. Elevated intracranial pressure (ICP) in children: Management - UpToDate
Indications for Intubation1
This is a clinical decision, there is no lab value that will define a need to intubate
Initial Ventilator Settings1
Hypercapnia is preferable to hyperinflation, and is tolerable in many cases to avoid more serious lung/airway trauma and complications.
References
1. Sean M Fox. Mechanical Ventilation for Severe Asthma. Pediatric EM Morsels. 7 November 2014. Mechanical Ventilation for Severe Asthma in Pediatrics (pedemmorsels.com)
1. Disconnect from Ventilator and allow chest to recoil
2. Consider Typical complications
3. Other Complications
References
1. Sean M Fox. Mechanical Ventilation for Severe Asthma. Pediatric EM Morsels. 7 November 2014. Mechanical Ventilation for Severe Asthma in Pediatrics (pedemmorsels.com)
2. Barry Brenner, Thomas Corbridge, Antoine Kazzi. Intubation and Mechanical Ventilation of the Asthmatic Patient in Respiratory Failure. Proceedings of the American Thoracic Society. 2009. 6(4) pp371-379. Intubation and Mechanical Ventilation of the Asthmatic Patient in Respiratory Failure | Proceedings of the American Thoracic Society (atsjournals.org)
|
S |
Setting Up |
|
|
|
P |
Perception of condition/seriousness |
|
|
|
I |
Invitation from the patient to give information |
|
|
|
K |
Knowledge: giving medical facts |
|
|
|
E |
Explore emotions and empathize |
|
|
|
S |
Strategy and Summary |
|
|
Adapted From: Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
| Empathetic Statements | Exploratory Questions | Validating Response |
| “I can see how upsetting this is to you.” | “How do you mean?” | “I can understand how you felt that way.” |
| “I can tell you weren't expecting to hear this.” | “Tell me more about it.” | “I guess anyone might have that same reaction.” |
| “I know this is not good news for you.” | “Could you explain what you mean?” | “You were perfectly correct to think that way.” |
| “I'm sorry to have to tell you this.” | “You said it frightened you?” | “Yes, your understanding of the reason for the tests is very good.” |
| “This is very difficult for me also.” | “Could you tell me what you're worried about?” | “It appears that you've thought things through very well.” |
| “I was also hoping for a better result.” | “Now, you said you were concerned about your children. Tell me more.” | “Many other patients have had a similar experience.” |
Source: Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
Recognizing an Inferior STEMI on an ECG1,2
Determining which artery is the culprit1
References
1. Ed Burns and Robert Buttner. Inferior STEMI. Life in the Fast Lane. 8 February 2021. Inferior STEMI • LITFL • ECG Library Diagnosis
2. Cardiac Care Network. STEMI Education for Emergency Department. CorHealth Ontario. ND. PowerPoint Presentation (corhealthontario.ca)
3. Huang et al. New ST-segment algorithms to determine culprit artery location in acutre inferior myocardial infarction. The American Journal of Family Medicine. Sep 2016. 34(9). pp1772-1778. https://doi.org/10.1016/j.ajem.2016.06.005
| Biochemical Criteria of DKA | |
| Hyperglycemia |
|
| Metabolic Acidosis |
|
| Ketosis |
|
| Assessing Severity of Pediatric DKA | ||||
| Defining Features | Severe | Moderate | Mild | |
| Venous pH | <7.1 | 7.1-<7.2 | 7.2-<7.3 | |
| Serum bicarbonate (mEq/L)* | <5* | 5-9 | 10-<15* | |
*For particularly vulnerable patients like young children or in resource-limited settings, these thresholds may be raised to heighten sensitivity
References
1. Nicole Glaiser. Diabetic Ketoacidosis in Children: Clinical Features and Diagnosis. UpToDate. 30 October 2020. UpToDate
2018 Canadian Diabetes Association DKA Guidelines treatment algorithm, adapted from https://guidelines.diabetes.ca/docs/CPG-2018-full-EN.pdf
Source: DKA Recognition and ED Management | Emergency Medicine Cases
Generally, you should avoid intubating a DKA patient, for several reasons:
Intubate if2:
When Intubating1:
References
1. Helman, A. Baimel, M. Sommer, L. Tillmann, B. Episode 146 – DKA Recognition and ED Management. Emergency Medicine Cases. September, 2020. https://emergencymedicinecases.com/dka-recognition-ed-management.
2. Josh Farkas. PulmCrit - Four DKA Pearls. PulmCrit (EMCrit). May 2014. PulmCrit - Four DKA Pearls (emcrit.org)
|
Potential Cause |
How to Identify |
Treatments |
|
Hypovolemia |
Rapid heart rate and narrow QRS on ECG; other symptoms of low volume |
Infusion of normal saline or Ringer’s lactate |
|
Hypoxia |
Slow heart rate |
Airway management and effective oxygenation |
|
Hydrogen ion excess (acidosis) |
Low amplitude QRS on the ECG |
Hyperventilation; consider sodium bicarbonate bolus |
|
Hypoglycemia* |
Bedside glucose testing |
IV bolus of dextrose |
|
Hypokalemia |
Flat T waves and appearance of a U wave on the ECG |
IV Magnesium infusion |
|
Hyperkalemia |
Peaked T waves and wide QRS complex on the ECG |
Consider calcium chloride, sodium bicarbonate, and an insulin and glucose protocol |
|
Hypothermia |
Typically preceded by exposure to a cold environment |
Gradual rewarming |
|
Tension pneumothorax |
Slow heart rate and narrow QRS complexes on the ECG; difficulty breathing |
Thoracostomy or needle decompression |
|
Tamponade – Cardiac |
Rapid heart rate and narrow QRS complexes on the ECG |
Pericardiocentesis |
|
Toxins |
Typically will be seen as a prolonged QT interval on the ECG; may see neurological symptoms |
Based on the specific toxin |
|
Thrombosis (pulmonary embolus) |
Rapid heart rate with narrow QRS complexes on the ECG |
Surgical embolectomy or administration of fibrinolytics |
|
Thrombosis (myocardial infarction) |
ECG will be abnormal based on the location of the infarction |
Dependent on extent and age of MI |
*Hypoglycemia is not officially one of the H’s and T’s for adults, but it still can be an important cause of PEA, especially in children. If another reversible cause has not been discovered or if the patient is known to be susceptible to hypoglycemia (e.g., brittle diabetes, past surreptitious use of insulin) then this potential cause of PEA should be considered.
|
S |
Setting Up |
|
|
|
P |
Perception of condition/seriousness |
|
|
|
I |
Invitation from the patient to give information |
|
|
|
K |
Knowledge: giving medical facts |
|
|
|
E |
Explore emotions and empathize |
|
|
|
S |
Strategy and Summary |
|
|
Adapted From: Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
| Empathetic Statements | Exploratory Questions | Validating Response |
| “I can see how upsetting this is to you.” | “How do you mean?” | “I can understand how you felt that way.” |
| “I can tell you weren't expecting to hear this.” | “Tell me more about it.” | “I guess anyone might have that same reaction.” |
| “I know this is not good news for you.” | “Could you explain what you mean?” | “You were perfectly correct to think that way.” |
| “I'm sorry to have to tell you this.” | “You said it frightened you?” | “Yes, your understanding of the reason for the tests is very good.” |
| “This is very difficult for me also.” | “Could you tell me what you're worried about?” | “It appears that you've thought things through very well.” |
| “I was also hoping for a better result.” | “Now, you said you were concerned about your children. Tell me more.” | “Many other patients have had a similar experience.” |
Source: Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
|
S |
Setting Up |
|
|
|
P |
Perception of condition/seriousness |
|
|
|
I |
Invitation from the patient to give information |
|
|
|
K |
Knowledge: giving medical facts |
|
|
|
E |
Explore emotions and empathize |
|
|
|
S |
Strategy and Summary |
|
|
Adapted From: Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
|
STOP for 5 Minutes |
|||
|
|||
|
Things to STATE FIRST:
|
|||
|
S |
Summarize the case |
|
|
|
T |
Things that went well |
|
|
|
O |
Opportunities to improve |
|
|
|
P |
Points to action and responsibilities |
|
|
Adapted From: Walker CA, McGregor L, Taylor C, Robinson S. STOP5: a hot debrief model for resuscitation cases in the emergency department. Clin Exp Emerg Med. 2020;7(4):259-266. doi:10.15441/ceem.19.086
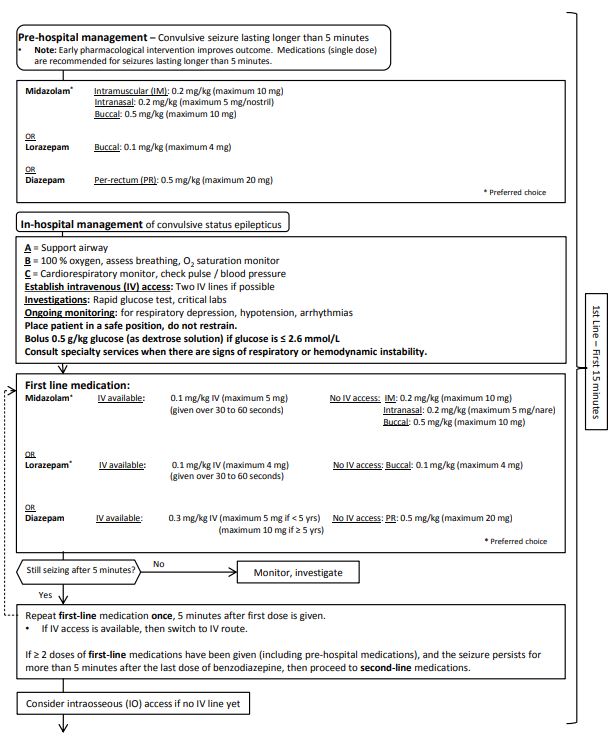

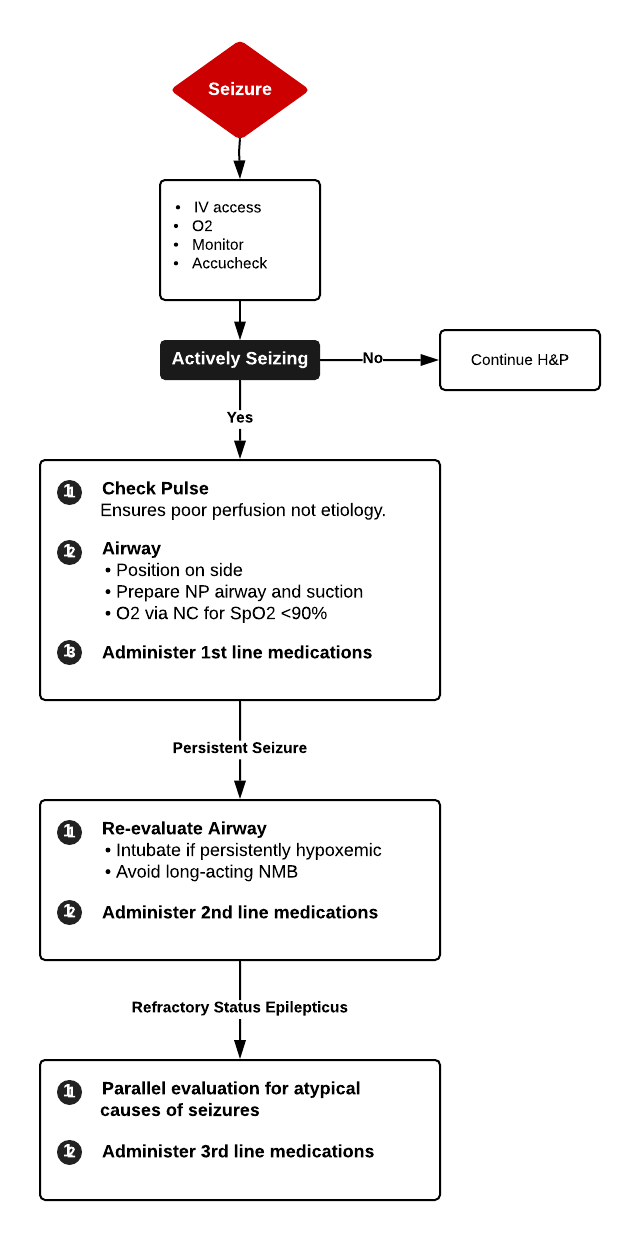
This algorithm can be found in CPS' position statement online here: https://cps.ca/documents/position/emergency-management-of-the-paediatric-patient-with-convulsive-status-epilepticus
The following are indicators of Opioid Overdose:
Reference: A Stolbach. 2022. Acute Opioid Intoxication in Adults. UpToDate.
It is important to collect laryngectomy and tracheostomy history from this patient because:
Laryngectomy History: If the patient has had their larynx removed, the upper airway is not connected to the trachea. Oral ventilation and oral intubation would thus be impossible. They would need to be ventilated and intubated through the stoma.
Tracheostomy History: If the tracheostomy is less than 7 days old, and the airway is patent (no laryngectomy), then oral intubation of the patient is preferred
Short Video: https://youtu.be/wmEwuc7Vs0w
Longer video: https://youtu.be/khS56oyBVFc
1. Total breech extraction should not be performed to deliver singleton breech.
2. Delivery of the breech wit hthe woman in the upright position, or in the all fours position, may reduce the need for intervention
3. Necessity of pushing in second stage of labour should be explained to the woman
4. Provide adequate analgesia. Be aware that dense epidural analgesia will hamper maternal pushing efforts
5. Spontaneous descent and expulsion to the umbilicus should occur with maternal pushing only: DO NOT PULL ON BREECH
6. Episiotomy may be considered once anterior buttock and anus are crowning
7. Spontaneous delivery of enture breech fetus is desirable. Delivery of aftercoming head may be facilitated by adequate maternal pushing efforts, oxytocin augmentation after delivery of fetal body or uterin fundal pressure. Assisted deivery is acceptable if there is delay in delivery. Following manoeuvres may be required:
a. Pinard's manoeuvre to deliver the fetal legs may be considered once popliteal fossae visible
b. Lovset's manoeuvre to deliver nuchal arms
8. Support baby to maintain head in a flexed position and body in a horizontal position. Delivery of the aftercoming head may be achieved with maternal pushing efforts alone. Oxytocin augmentation or uterin fundal pressure can be used to treat expulsive delay after the breech has crowned.
9. Failing these, the Mauriceau-Smellie-Viet manoeuvre, or Piper forceps, may be required to deliver head in flexion
Source:
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
1. Insert two fingers along one leg to the knee
2. Abduct knee away from midline while flexing the leg at the hip
3. This will cause spontaneous flexion of the knee and delivery of the foot
4. Knees of frank breech are hyperextended, and it is important to correctly identify popliteal fossae to avoid further hyperextension
Source:
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.

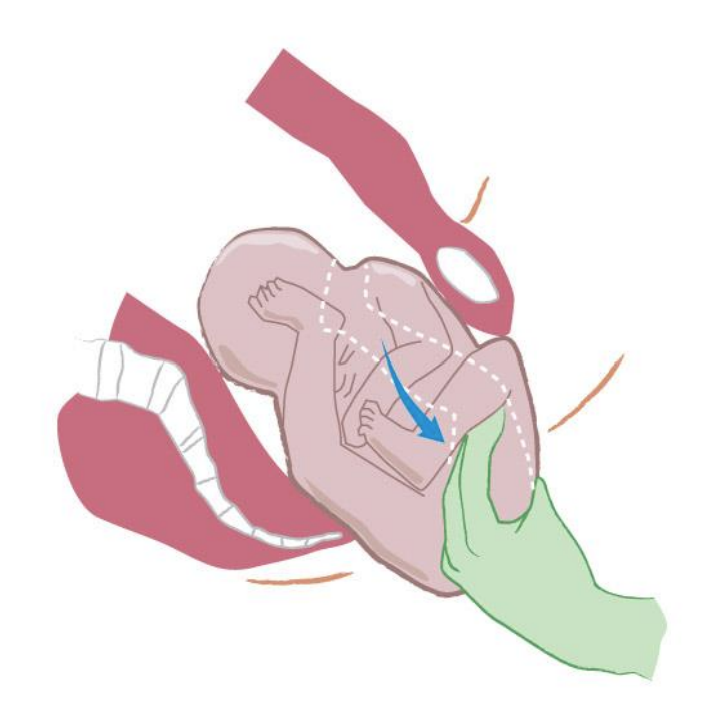
A1. Grasp fetus by bony pelvis with 2 hands and raise towards maternal pubic symphisis
A2. Turn fetal torso while lowering it to bring shoulder underneath pubic symphisis
B1. Sweep humerus of posterior arm across chest to release
A3. Rotate fetal trunk back through a sacrum-anterior position to the other side
B2. Sweep humerus of remaining arm across chest to release
Source:
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
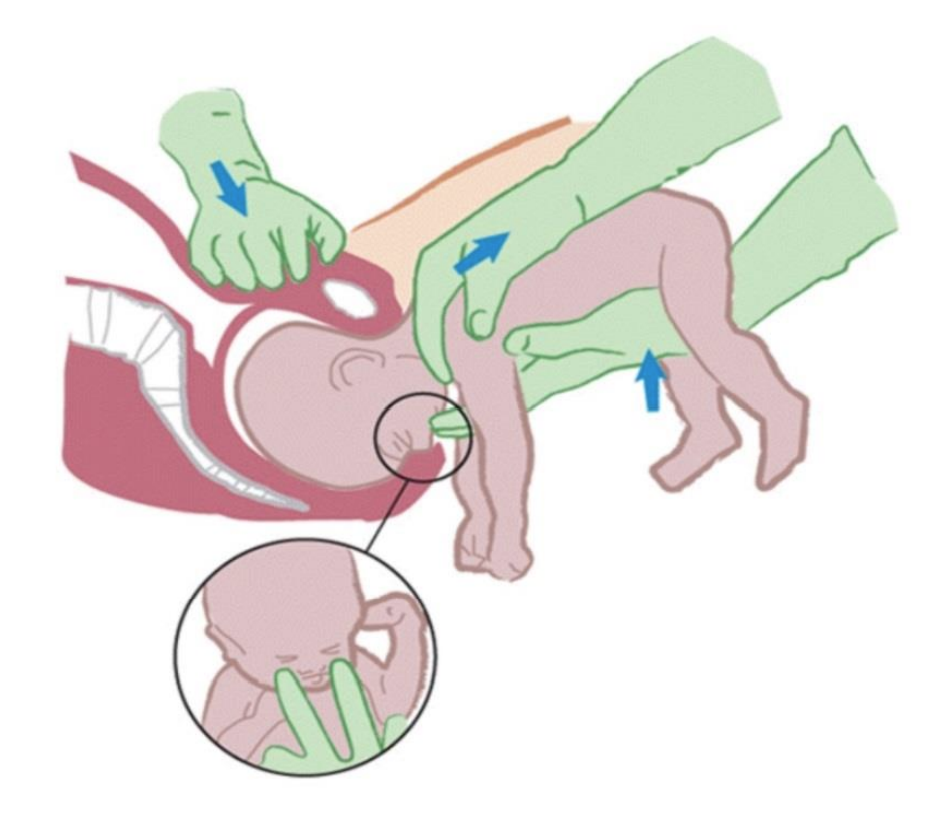
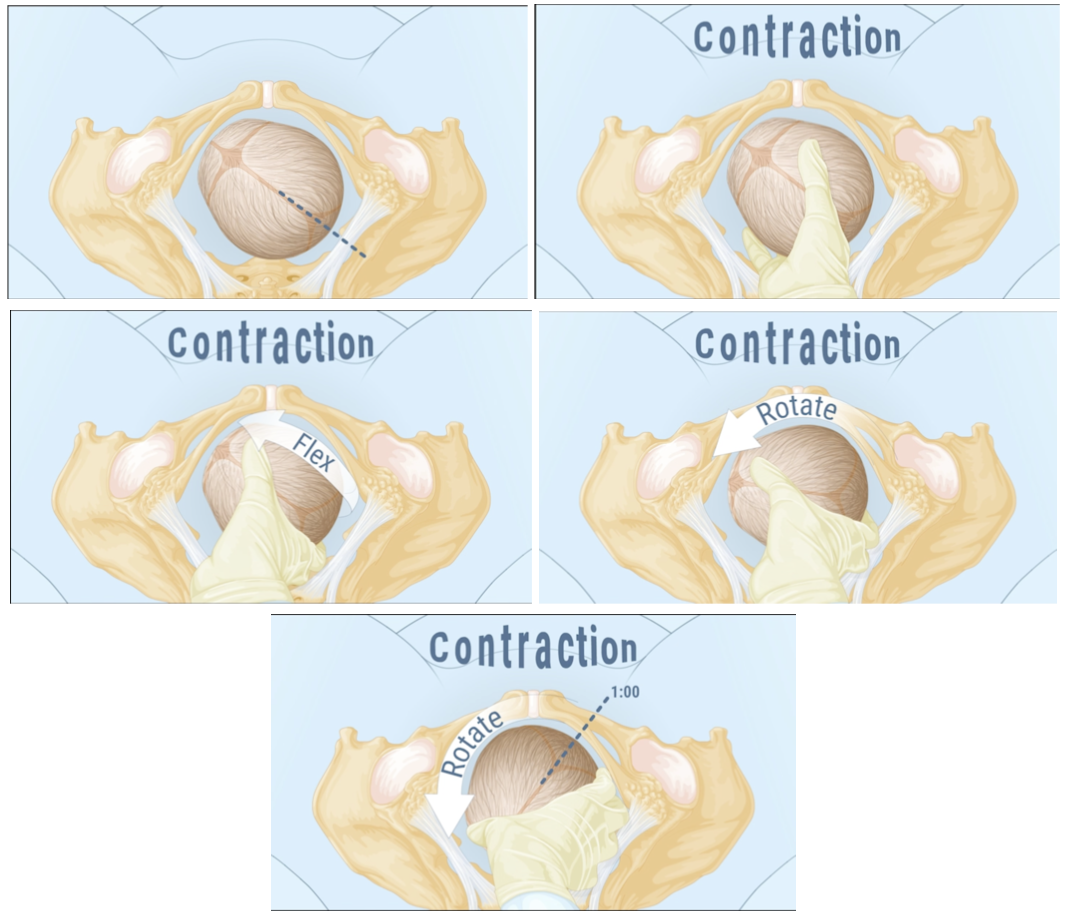
1. Place one hand underneath fetus and palpate the fetal maxilla. Have assistant maintain suprapubic pressure.
2. Apply pressure to fetal maxilla to flex head
3. Grasp fetal shoulders with other hand to apply gentle traction
4. Maintain flexion of head and suprapubic pressure while applying traction to aid delivery
Source
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
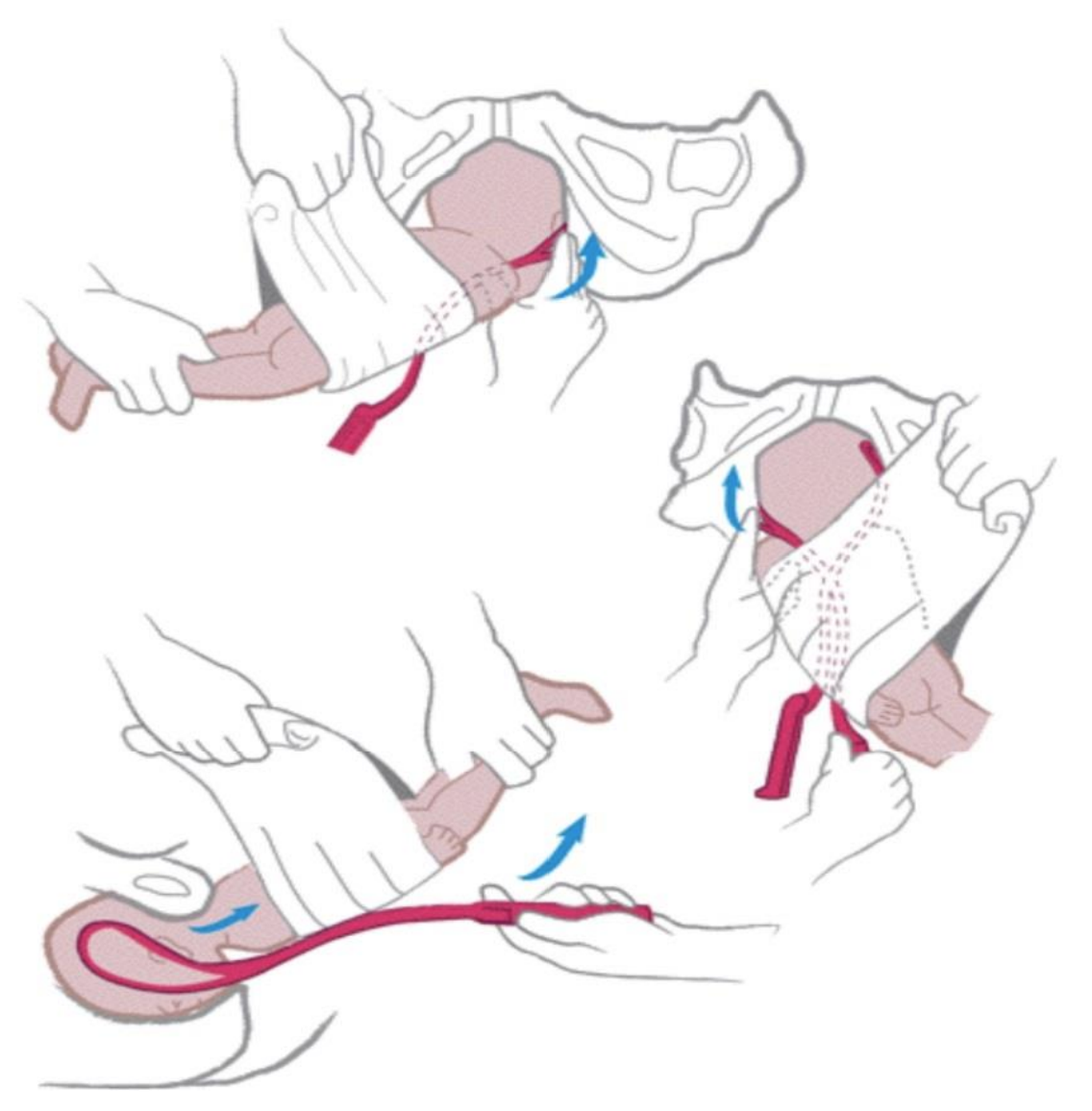
1. Elevate fetal body using warm towel
2. Apply left blade of forceps to aftercoming head
3. Apply right blade of forceps with body still elevated
4. With body still elevated, use forceps to deliver head
Source:
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Created using information from: Simon LV, Hashmi MF, Bragg BN. APGAR Score. StatPearls. 2022 Feb. https://www.ncbi.nlm.nih.gov/books/NBK470569/
There are two equations that can be used to calculate the anion gap. It is common practice to use the second one, but the first is more accurate:
1. Na+ + K+ - Cl- - HCO3-
2. Na+- Cl- - HCO3-
Normal anion gap when including K+ is 12-20meEQ/L1
When not including K+, normal anion gap is 12 + 41
DDx of Elevated Anion Gap - MUDPILES Mnemonic1
M - Methanol, Metformin
U- Uremia
D - DKA
P - Paraldehyde, phenformin
I - Iron, INH, Ibuprofen (large ingestions)
L - Lactic Acidosis
E - Ethylene Glycol
S - Salicylates
Other possibilities: Starvation/ETOH ketoacidosis, Carbon monoxide, CN poisoning, Colchicine, Toluene, Chronic acetaminophen use
References:
1. Fields A, Iacomini P, Cunningham R, Miller CM, Ross J, Lu K, Davey M, Young N, Ostermayer D, Donaldson R. Anion Gap. WikEM. Feb 2021. wikem.org/wiki/Anion_gap
Inclusion Criteria - Only apply to patients with GCS 13-15 and at least one of the following:
Exclusion Criteria - If any of the following are true, Canadian CT Head Rules do not apply:
Medium Risk Criteria - Presence of one or more indicate medium risk for brain injury on CT
High Risk - Presence of one or more indicate high risk for brain injury on CT and possible need for neurological
Source: MD Calc

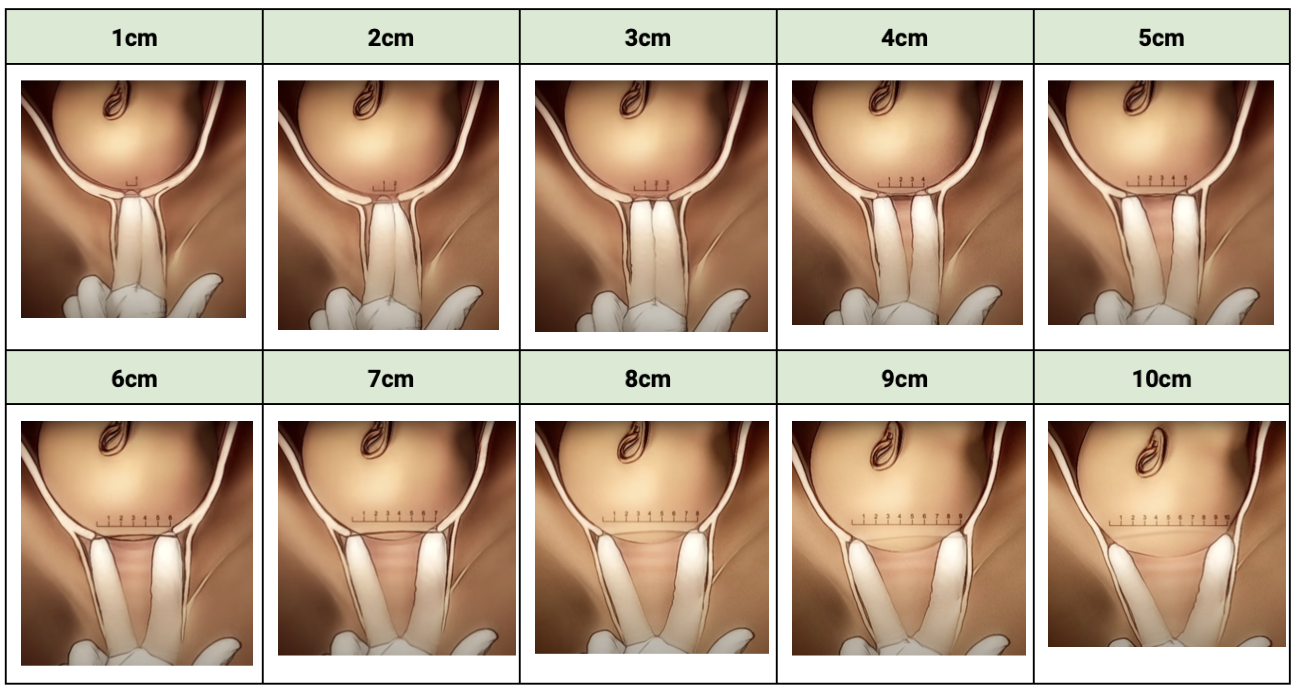
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/

Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M

Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Reference(s):
Argani, A. H., & Satin, A. J. (2022). Occiput Posteror Position. In Barss V (Ed.), UpToDate. Retrieved Aug 20, 2023, from https://www.uptodate.com/contents/occiput-posterior-position?search=occiput%20posterior%20position&source=search_result&selectedTitle=1~13&usage_type=default&display_rank=1#references
Reference(s):
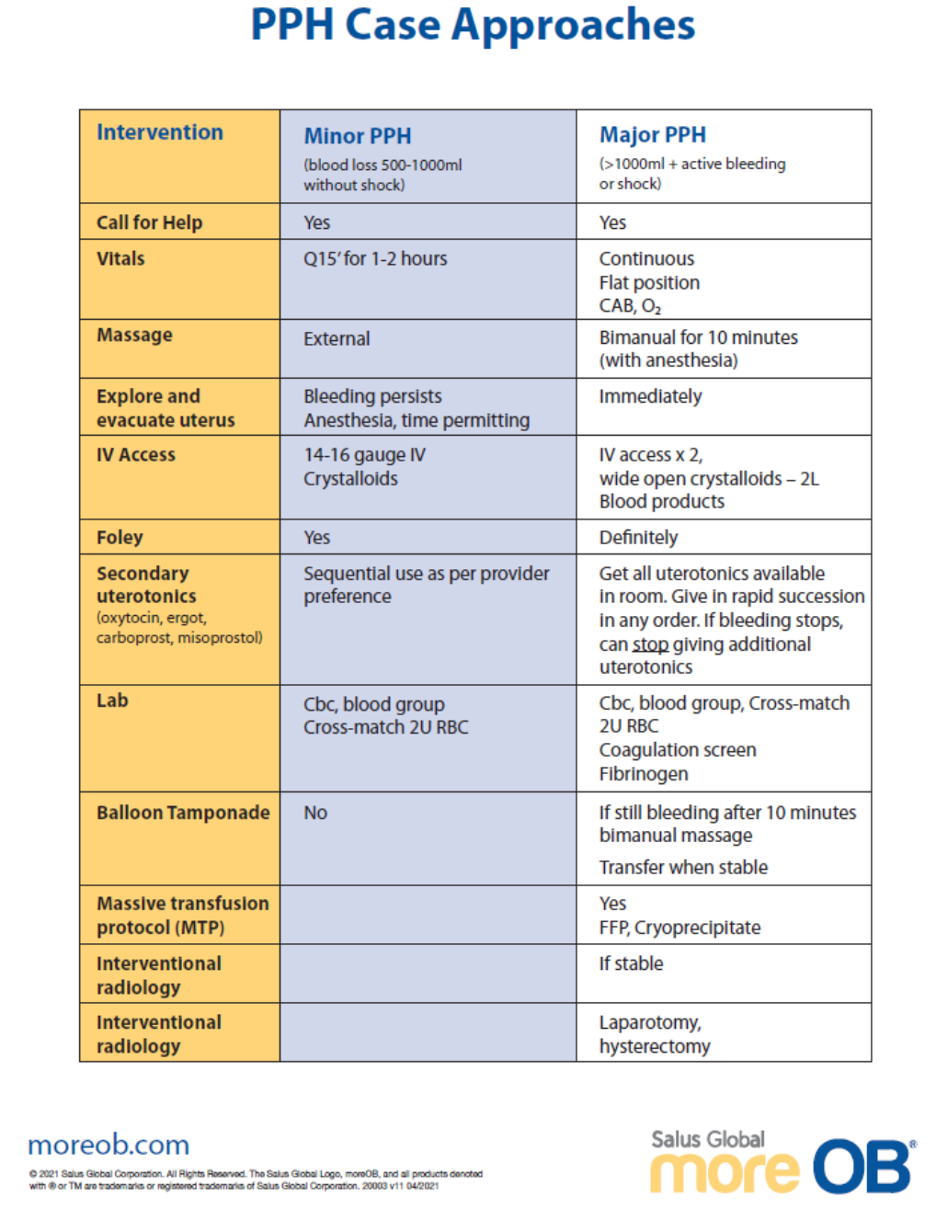
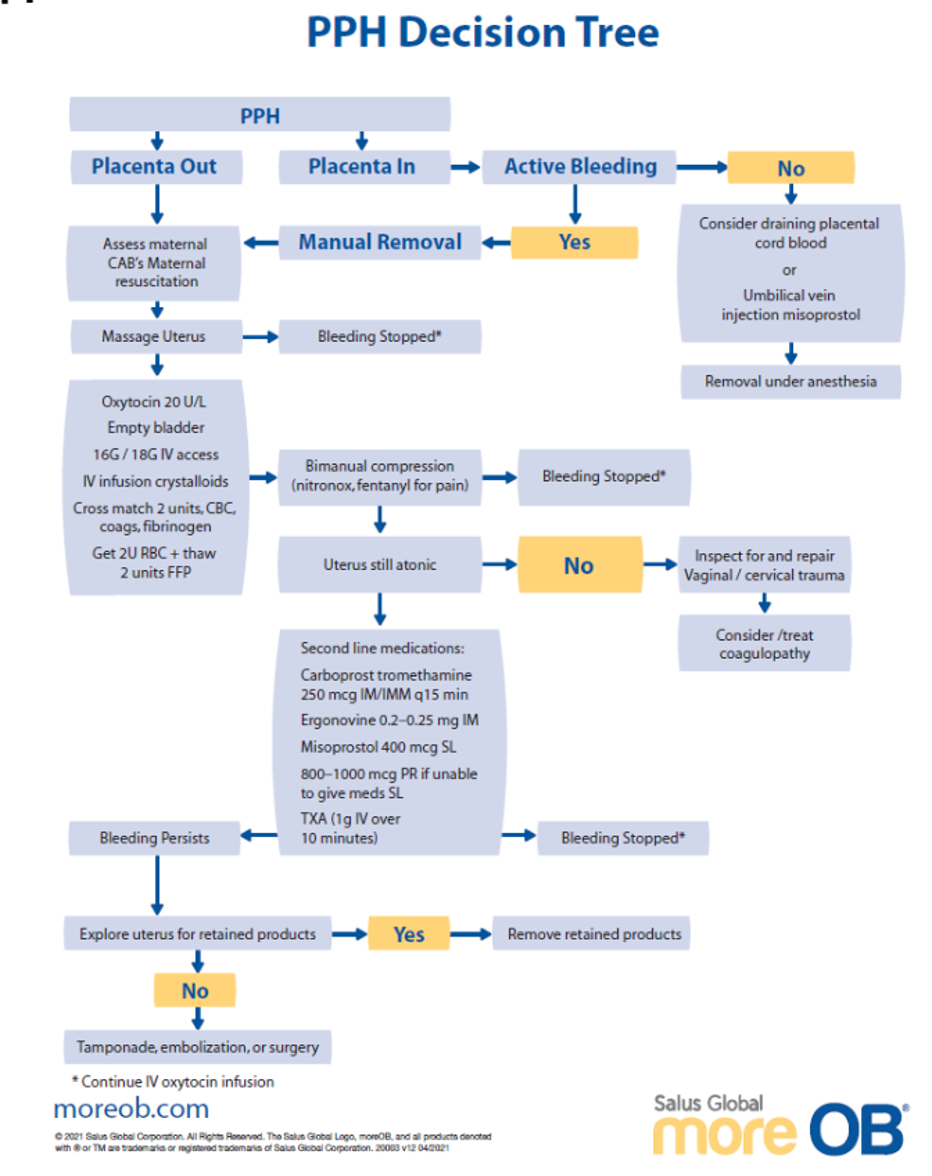
Retrieved July 5, 2023 from https://www.amboss.com/us/knowledge/postpartum-hemorrhage/
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.

Reference(s):
Retrieved January 4, 2024 from https://www.doctorstock.com/image/I0000pff4Hvr0dFc
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Reference(s):
Retrieved July 5, 2023 from https://www.amboss.com/us/knowledge/postpartum-hemorrhage/
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380

Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.

Classification of Placental Abruption:
| Abruption | Definition | Management |
| Mild | Abruption with no fetal compromise |
|
| Moderate | Abruption with fetal compromise |
|
| Severe | Abruption with fetal death |
|

Retrieved July 5, 2023 from https://www.amboss.com/us/knowledge/antepartum-hemorrhage
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
| Do Not 1. Pull, on the head 2. Push, on the fundus 3. Pivot or rotate the head 4. Panic |
|
| ALARMER Mneumonic for Shoulder Dystocia Management Note: Ask the woman to push after each maneuver. Avoid pushing between contractions while maneuvers are carried out to maximize cerebral perfusion. |
|
| A: Ask for help |
|
| L: Lift/Hyperflex legs |
McRoberts Maneuver |
| A: Anterior Shoulder Disimpaction | Abdominal Approach 1. Assistant applies steady or rocking suprapubic pressure with heel of clasped hands from the posterior aspect of the anterior shoulder to dislodge it. 2. Attempt with McRoberts maneuver.
Vaginal Approach (Rubin Maneuver) |
| R: Rotation of the posterior shoulder |
Woods Maneuver (Screw-like Maneuver)
|
| M: Manual removal of the posterior arm |
The arm is usually flexed at the elbow. If the arm is NOT flexed, Alternate maneuver or if the posterior hand cannot be reached, deliver the posterior shoulder using axillary traction: |
| E: Episiotomy | Note: An episiotomy may facilitate the Woods maneuver or manual removal of the posterior arm by creating more space. However, shoulder dystocia is NOT caused by obstructing soft tissue, therefore, performing an episiotomy on its own will not relieve a shoulder dystocia. |
| R: Roll over onto "all fours" |
Gaskin's Maneuver 2. Apply gentle downward pressure on the posterior shoulder of the fetus. |
|
Last Resort:
|
|
Videos:
Shoulder Dystocia & ALARMER Mnemonic (8.5 min.): https://youtu.be/BvkKMwDaryg
ALARMER Mnemonic (8.5 min.): https://youtu.be/jNmSJDbTARw
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Created using information from: Simon LV, Hashmi MF, Bragg BN. APGAR Score. StatPearls. 2022 Feb. https://www.ncbi.nlm.nih.gov/books/NBK470569/
| Signs of Placental Separation | |
|
1. Gush of blood |
|
| Active Management | |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
Contraindications to planned vaginal delivery breech. |
|
Contraindications to planned vaginal delivery breech.
|
|
Breech Delivery Technique Notes |
|
Delivery Technique
In the rare circumstance of a trapped aftercoming head or irreducible nuchal arms perform a symphysiotomy or Zavanelli maneuver. |
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
Pinard’s Maneuver: deliver fetal legs once the popliteal fossae are visible.
1. Insert two fingers along one leg to the knee. Note: The knees of a frank breech are hyperextended at this point. It is important to correctly identify the popliteal fossae to avoid further hyperextension and damage to the fetal knee. |
|
Bracht’s Maneuver: suprapubic pressure with the extension of the fetal neck.
|
|
Bickenbach Maneuver: reduction of the nuchal arms.
Release of the posterior arm. Release of the anterior arm. |
|
Løvset’s Maneuver: reduction of the nuchal arms.
Release of the posterior arm. Release of the first arm brings the other arm posteriorly. |
|
Mauriceau-Smellie-Veit Maneuver: delivery of the aftercoming head.
Note: As the fetal head is being delivered, flexion of the head is maintained by suprapubic pressure provided by an assistant, and simultaneously by pressure on the maxilla (inset) by the operator as traction is applied. |
|
Piper forceps: delivery of the aftercoming head.
Note: The blue arrows show the direction of movement. The fetal body is elevated using a warm towel and the left blade of the forceps is applied to the aftercoming head. The right blade is applied with the body still elevated. |
Videos:
Breech Delivery Technique (4 min): https://youtu.be/d9pU_6LDVUM
In-depth Technique Explanations (12 min) – Includes Piper Forceps Delivery: https://youtu.be/xOqWT06qVS8
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)
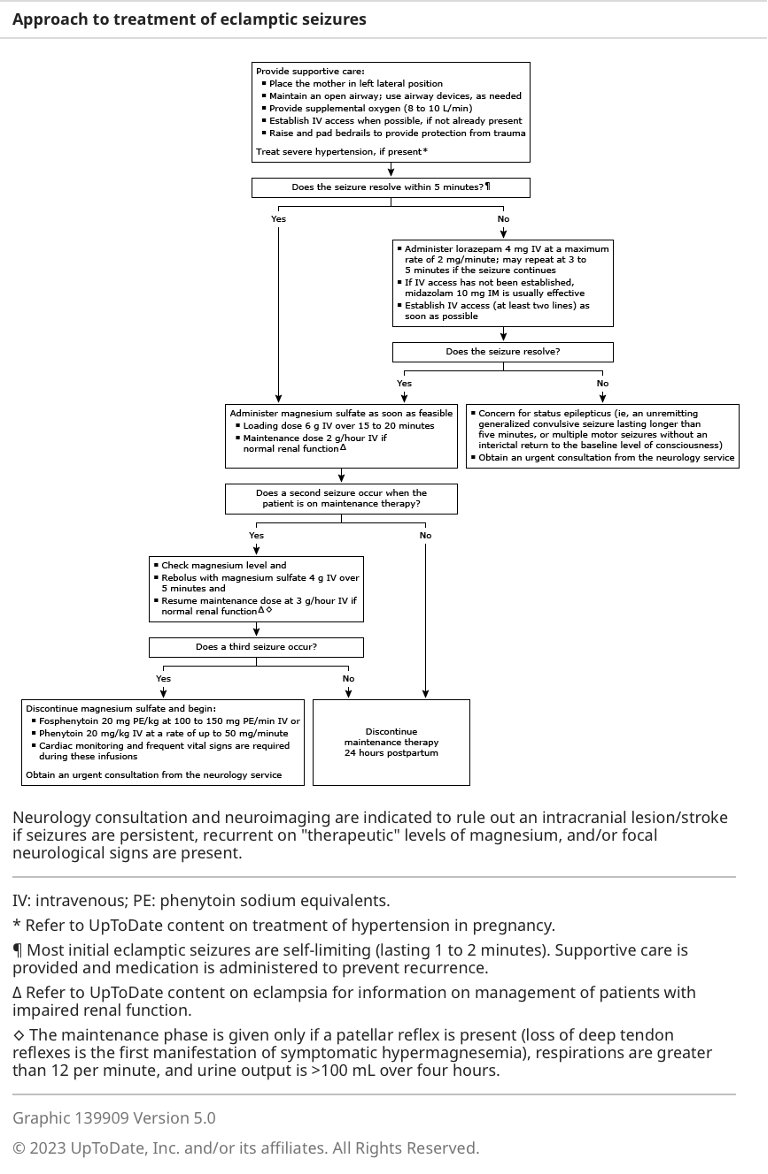
Norwitz E. R. (2022). Eclampsia. In Barss V (Ed.), UpToDate. Retrieved July 4, 2023, from https://www.uptodate.com/contents/eclampsia
Brandt-Andrews Maneuver (preferred): an abdominal hand secures the uterine fundus to hold it in a fixed position and prevent uterine inversion while the other hand exerts sustained downward traction on the clamped umbilical cord.
Reference(s):
Anderson, Janice M, and Duncan Etches. 2007. Prevention and Management of Postpartum Hemorrhage. www.aafp.org/afp. (October 12, 2023).
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)

Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine 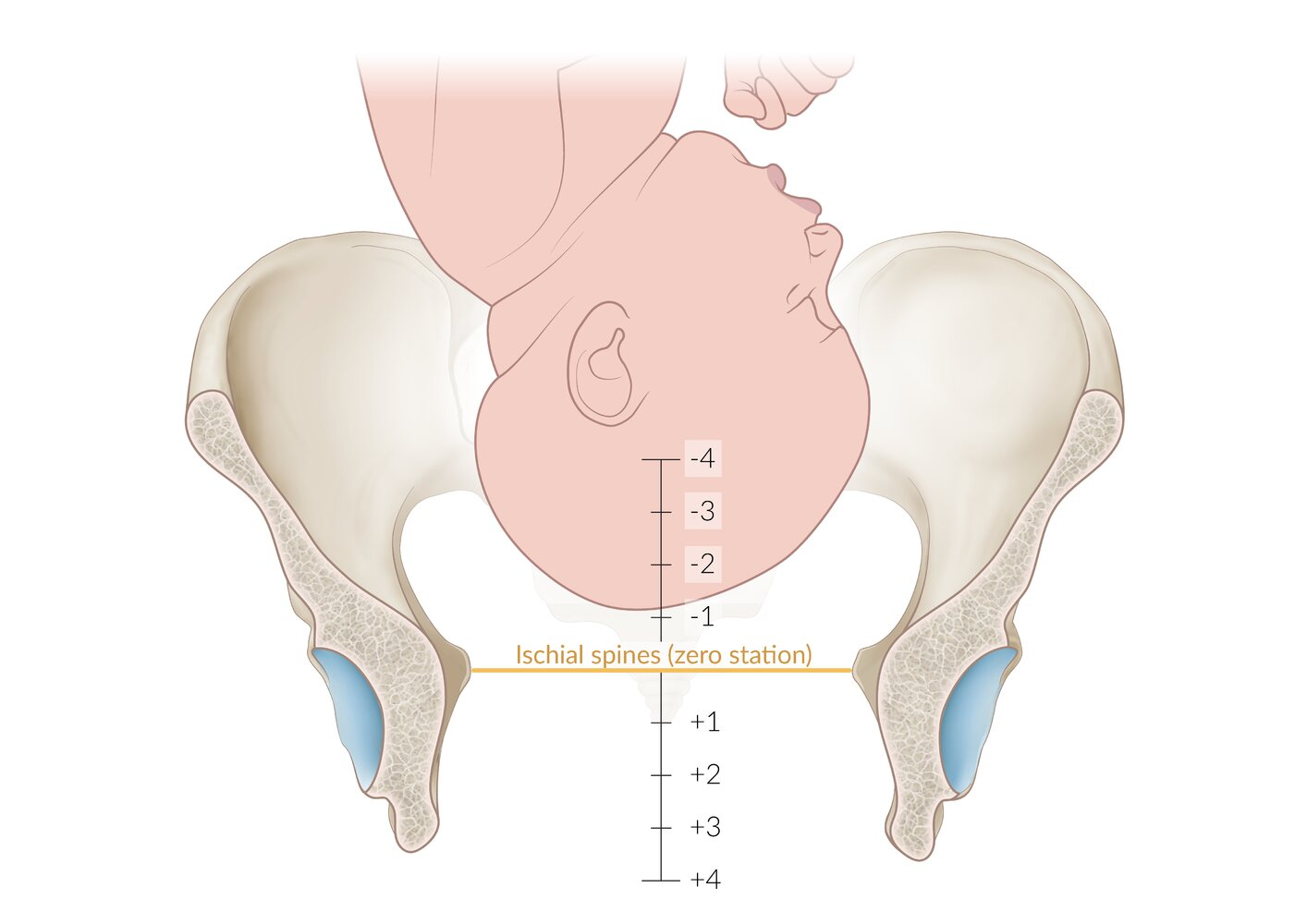 |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level 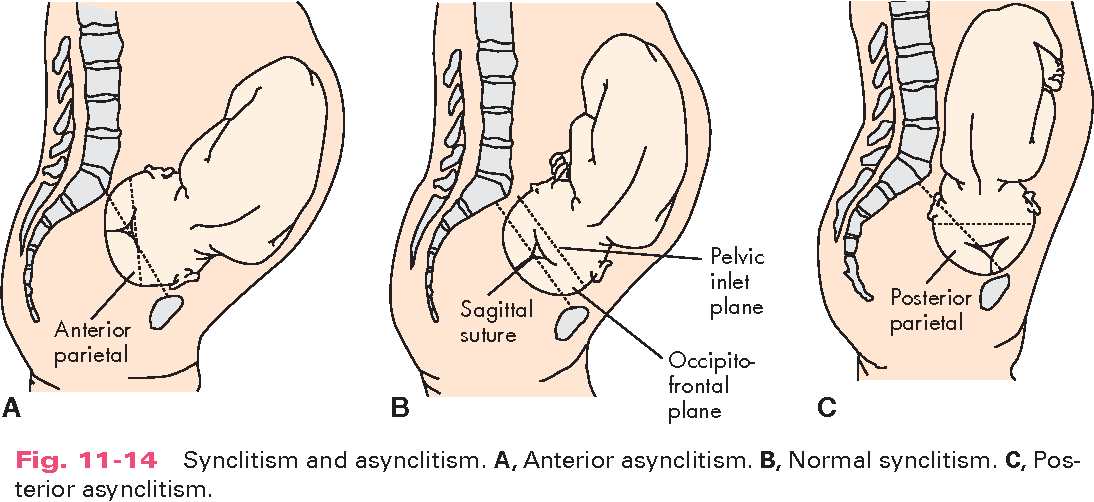 |
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
Compress the uterus against the anterior part of the cervix with a hand in the vagina and a hand on the fundus.

Retrieved July 20, 2023 from Bromberek, Elaine & Smereck, Janet. (2017). Evaluation and Treatment of Postpartum Hemorrhage. 10.1007/978-3-319-54410-6_8.
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| Signs of Placental Separation | |
|
1. Gush of blood |
|
| Active Management | |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
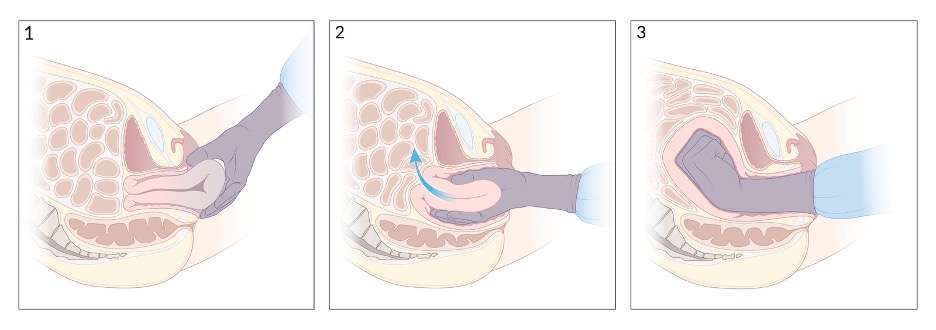
Compress the uterus against the anterior part of the cervix with a hand in the vagina and a hand on the fundus.
Retrieved July 20, 2023 from Bromberek, Elaine & Smereck, Janet. (2017). Evaluation and Treatment of Postpartum Hemorrhage. 10.1007/978-3-319-54410-6_8.
Perform external aortic compression with the non-pneumatic anti-shock garment (NASG).
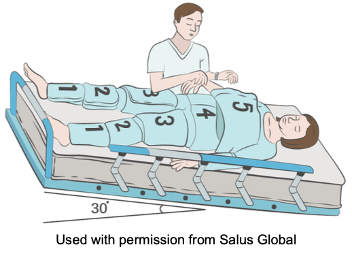
Manual compression of the aorta by standing on the woman's left and using one's right fist to compress the aorta and using one's left hand to feel for the loss of the femoral pulse.

Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Brandt-Andrews Maneuver (preferred): an abdominal hand secures the uterine fundus to hold it in a fixed position and prevent uterine inversion while the other hand exerts sustained downward traction on the clamped umbilical cord.
Reference(s):
Anderson, Janice M, and Duncan Etches. 2007. Prevention and Management of Postpartum Hemorrhage. www.aafp.org/afp. (October 12, 2023).
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)

Sobel J. D. (2022). Bacterial vaginosis: Initial Treatment. In Eckler K (Ed.), UpToDate. Retrieved July 12, 2023, from https://www.uptodate.com/contents/bacterial-vaginosis-initial-treatment
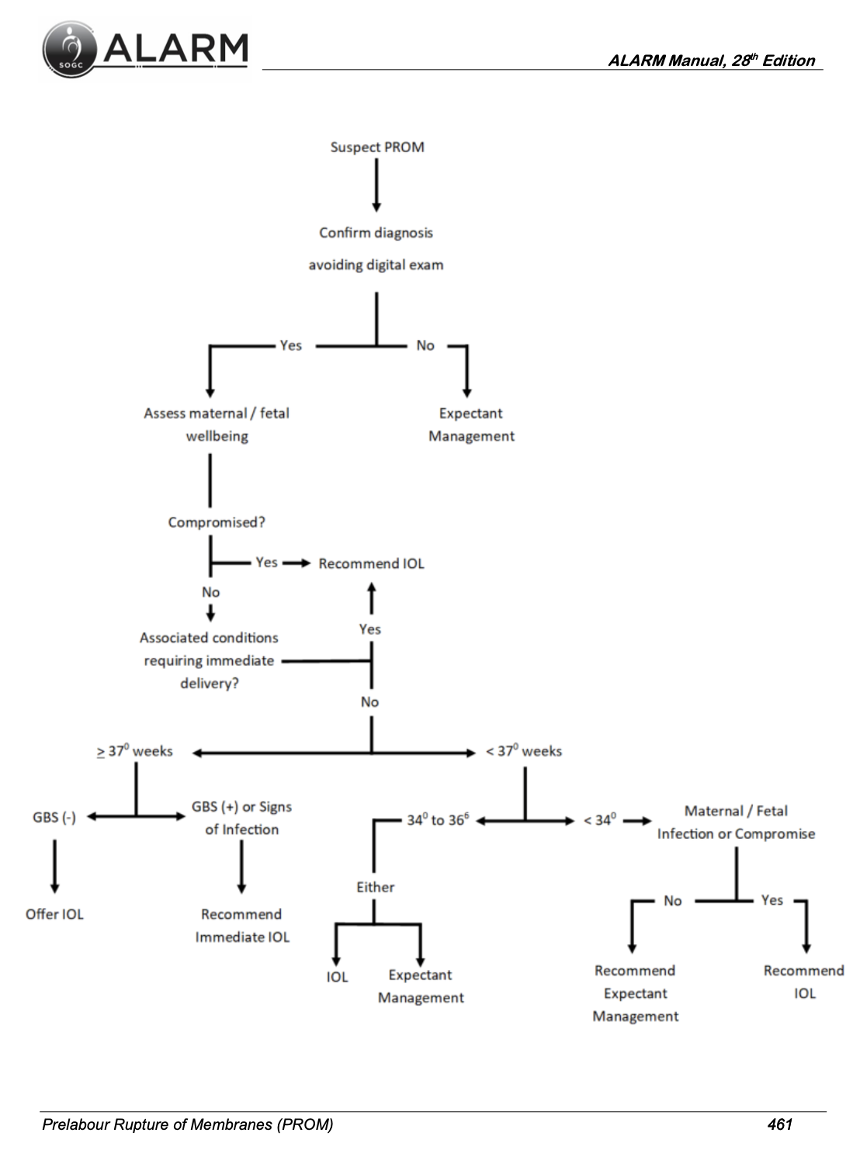
Administration recommendations for those identified as candidates for vaginal progesterone:
Discontinuation between 34-36 weeks may be individualized depending on clinical situation and discussion of potential benefits. The use of progestogen does NOT prolong pregnancy in singleton gestations with preterm prelabour rupture of membranes.
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
S: Antenatal Corticosteroid Therapy |
Options:
Considerations: Contraindications: Active tuberculosis, gastric ulcers, and chorioamnionitis
|
|
T: Tocolytics |
|
Contraindications:
See tocolytic administration chart below. |
|
A: Antibiotics and GBS Prophylaxis |
|
Antepartum Management:
PPROM (<34 Weeks Gestation) – Antibiotic Treatment to reduce risk of chorioamnionitis, prolong the latency period, and reduce neonatal morbidity. · Option 1: Ampicillin (2g IV q6h) and Erythromycin (250mg IV q6h) for 48 hours, followed by Amoxicillin (250mg PO, q8h) and Enteric-Coated Erythromycin Base (333mg PO q8h) for 5 days (Mercer protocol) · Option 2: Erythromycin (250mg PO q6h for 10 days) · Option 3: Clarithromycin or Azithromycin in appropriate doses (below) Do NOT administer amoxicillin with clavulanic acid (increased risk of necrotizing enterocolitis in the presence of PROM). Intrapartum Management:
Membrane Rupture or Onset of Active Labour: Administer to all women with (1) previous infant with invasive GBS disease, (2) GBS bacteriuria during current pregnancy, (3) positive screening culture within the past five weeks. If GBS status is unknown: Administer for (1) preterm labour (<37 weeks), (2) rupture of membranes for >18h, (3) maternal fever >38 degrees Celsius. NOT Indicated: (1) Planned Caesarean Section (CS) in the absence of labour or membrane rupture (regardless of GBS status) and (2) Negative vaginal and rectal GBS screening culture within five weeks. Preterm labour with intact membranes:
Prelabour rupture of membranes (PROM) and preterm PROM (PPROM):
|
|
T: Transport |
Considerations: Availability at referral centre, time, and conditions (e.g., weather), stability of mother and fetus, and risk of delivery en route (response to tocolytics, presentation, etc.). Contraindications: Imminent delivery, no experienced attendants to accompany mother, adverse weather, and/or travel hazards. |
|
Calcium Channel Blockers (nifedipine) |
PG Synthetase Inhibitors (indomethacin) |
Nitroglycerin |
|
Evidence:
Findings:
Dose:
Side Effects:
|
Evidence:
Findings:
Dose:
Side Effects:
|
There is limited evidence of the benefit of nitroglycerin for tocolysis. |
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Note(s):
· Antenatal magnesium sulphate administration should be considered for neuroprotection for woman with imminent preterm birth (<33 weeks).
· If magnesium sulphate has been started, tocolysis should be discontinued.
· Discontinue if delivery is no longer imminent or a maximum of 24 hours after therapy has been administered.

|
Signs of Magnesium (Mg) Toxicity – correlates with the serum Mg concentration, uncommon in patients with good renal function. |
|
|
SIGN |
Serum Mg Concentration |
|
Loss of Deep Tendon Reflexes |
7-10 mEq/L (8.5-12 mg/dL or 3.5-5 mmol/L) |
|
Respiratory Paralysis |
10-13 mEq/L (12-16 mg/dL or 5-6.5 mmol/L) |
|
Cardiac conduction altered |
>15 mEq/L (>18 mg/dL or >7.5 mmol/L) |
|
Cardiac Arrest |
>25 mEq/L (>30 mg/dL or >12.5 mmol/L) |
|
Antidote: Calcium Gluconate, 15-30 mL of 10% solution (1500-3000 mg) IV over 2-5 minutes in patients in cardiac arrest or severe cardiac toxicity related to hypermagnesemia.
|
|
Norwitz E. R. (2023). Preeclampsia: Intrapartum and postpartum management and long-term prognosis. In Barss V (Ed.), UpToDate. Retrieved July 11, 2023, from https://www.uptodate.com/contents/preeclampsia-intrapartum-and-postpartum-management-and-long-term-prognosis
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
S: Antenatal Corticosteroid Therapy |
Options:
Considerations: Contraindications: Active tuberculosis, gastric ulcers, and chorioamnionitis
|
|
T: Tocolytics |
|
Contraindications:
See tocolytic administration chart below. |
|
A: Antibiotics and GBS Prophylaxis |
|
Antepartum Management:
PPROM (<34 Weeks Gestation) – Antibiotic Treatment to reduce risk of chorioamnionitis, prolong the latency period, and reduce neonatal morbidity. · Option 1: Ampicillin (2g IV q6h) and Erythromycin (250mg IV q6h) for 48 hours, followed by Amoxicillin (250mg PO, q8h) and Enteric-Coated Erythromycin Base (333mg PO q8h) for 5 days (Mercer protocol) · Option 2: Erythromycin (250mg PO q6h for 10 days) · Option 3: Clarithromycin or Azithromycin in appropriate doses (below) Do NOT administer amoxicillin with clavulanic acid (increased risk of necrotizing enterocolitis in the presence of PROM). Intrapartum Management:
Membrane Rupture or Onset of Active Labour: Administer to all women with (1) previous infant with invasive GBS disease, (2) GBS bacteriuria during current pregnancy, (3) positive screening culture within the past five weeks. If GBS status is unknown: Administer for (1) preterm labour (<37 weeks), (2) rupture of membranes for >18h, (3) maternal fever >38 degrees Celsius. NOT Indicated: (1) Planned Caesarean Section (CS) in the absence of labour or membrane rupture (regardless of GBS status) and (2) Negative vaginal and rectal GBS screening culture within five weeks. Preterm labour with intact membranes:
Prelabour rupture of membranes (PROM) and preterm PROM (PPROM):
|
|
T: Transport |
Considerations: Availability at referral centre, time, and conditions (e.g., weather), stability of mother and fetus, and risk of delivery en route (response to tocolytics, presentation, etc.). Contraindications: Imminent delivery, no experienced attendants to accompany mother, adverse weather, and/or travel hazards. |
|
Calcium Channel Blockers (nifedipine) |
PG Synthetase Inhibitors (indomethacin) |
Nitroglycerin |
|
Evidence:
Findings:
Dose:
Side Effects:
|
Evidence:
Findings:
Dose:
Side Effects:
|
There is limited evidence of the benefit of nitroglycerin for tocolysis. |
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Note(s):
· Antenatal magnesium sulphate administration should be considered for neuroprotection for woman with imminent preterm birth (<33 weeks).
· If magnesium sulphate has been started, tocolysis should be discontinued.
· Discontinue if delivery is no longer imminent or a maximum of 24 hours after therapy has been administered.
|
Signs of Magnesium (Mg) Toxicity – correlates with the serum Mg concentration, uncommon in patients with good renal function. |
|
|
SIGN |
Serum Mg Concentration |
|
Loss of Deep Tendon Reflexes |
7-10 mEq/L (8.5-12 mg/dL or 3.5-5 mmol/L) |
|
Respiratory Paralysis |
10-13 mEq/L (12-16 mg/dL or 5-6.5 mmol/L) |
|
Cardiac conduction altered |
>15 mEq/L (>18 mg/dL or >7.5 mmol/L) |
|
Cardiac Arrest |
>25 mEq/L (>30 mg/dL or >12.5 mmol/L) |
|
Antidote: Calcium Gluconate, 15-30 mL of 10% solution (1500-3000 mg) IV over 2-5 minutes in patients in cardiac arrest or severe cardiac toxicity related to hypermagnesemia.
|
|
Norwitz E. R. (2023). Preeclampsia: Intrapartum and postpartum management and long-term prognosis. In Barss V (Ed.), UpToDate. Retrieved July 11, 2023, from https://www.uptodate.com/contents/preeclampsia-intrapartum-and-postpartum-management-and-long-term-prognosis
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| FHR Pattern (VEAL) | Cause (CHOP) | Management (MINE) | |||
| V | Variable Deceleration | C | Cord Compression | M | Maternal Repositioning |
| E | Early Deceleration | H | Head Compression | I | Identify Labour Progress |
| A | Acceleration | O | Okay! | N | No Intervention |
| L | Late Deceleration | P | Placental Insufficiency | E | Evaluate (reposition, fluids, oxygen, emergency delivery). |
Retrieved July 17, 2023, from Melbourne University Obstetrics and Gynecology Society (Facebook)
Maternal Fever
Suspected Triple I
Confirmed triple I
Chen, K. T. Intrapartum fever. In: UpToDate, Barss V. A. (Ed), UpToDate, Waltham, MA, 2023.
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
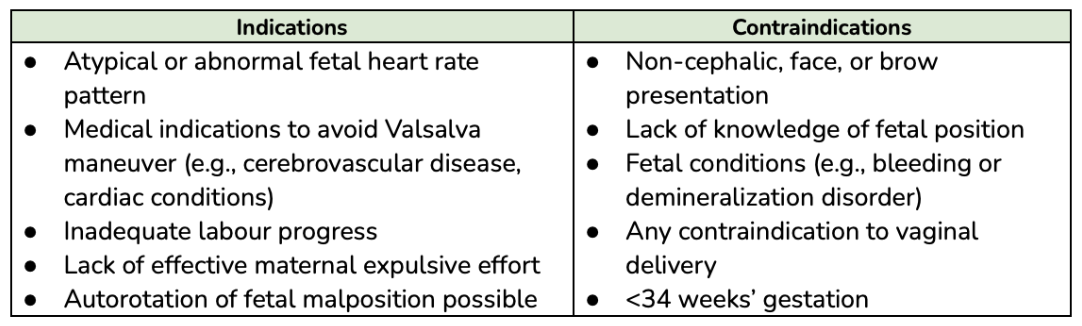
|
Indications |
|
|
High Priority |
|
|
Other Indications |
|
|
Contraindications |
Risks |
|
|
Prevention Strategies (to reduce induction for post-term):
Inducing Labour: Pros and Cons of Membrane Sweep (7.5 min): https://youtu.be/I5AlkgUvPZY?t=57
Membrane Sweep (2.5 min): https://youtu.be/GOqIJdysn1g
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Retrieved July 13, 2023, from https://slideplayer.com/slide/7908096/
Retrieved July 13, 2023, from https://doi.org/10.1016/j.jogc.2022.11.009
|
Induction of Labour: Pharmacologic Options Agents Include:
General Prostaglandin Note(s):
Adverse reactions:
|
|
|
Prostaglandin E2 (Dinoprostone) – Intravaginal OR Intracervical Gel |
|
|
|
|
Intravaginal (Posterior Fornix) |
Intracervical |
|
|
|
Prostaglandin E1 (Misoprostol) |
|
Eligibility: Indication for IOL, >35 Weeks Gestation Caution: Multiparous (>6 prior vaginal deliveries), Fetal Growth restriction or oligohydramnios Exclusion Criteria: <35 Weeks Gestation, Previous CS (or significant uterine surgery), Abnormal Fetal Heart Tracing, Regular or Painful Contractions |
|
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
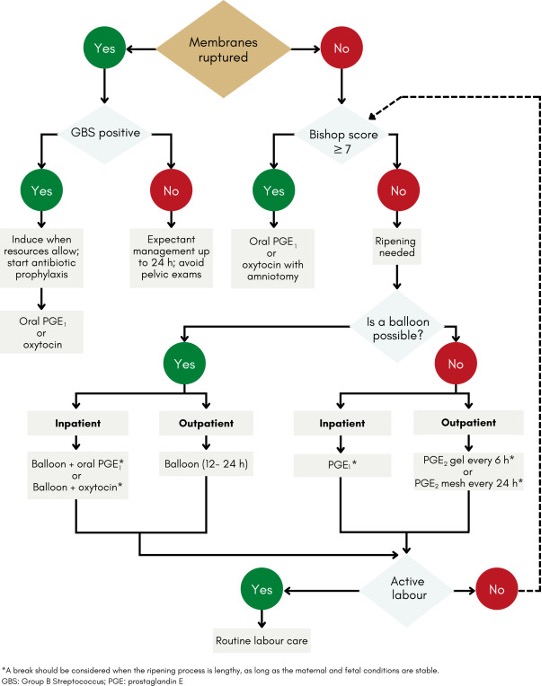
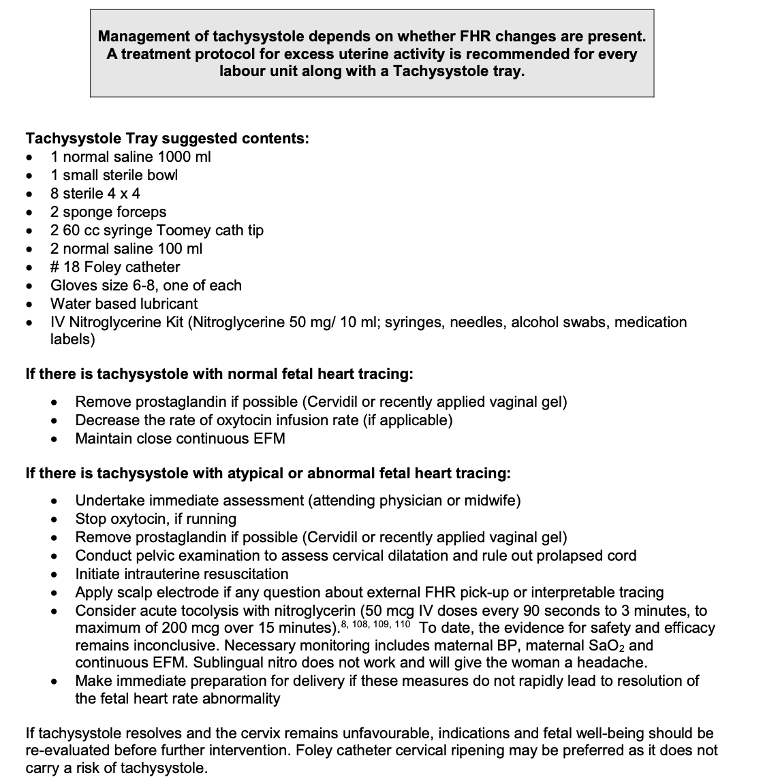
Note(s): Tachysystole is the term used to describe excessive uterine activity:
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
Antibiotics and GBS Prophylaxis |
|
Antepartum Management:
PPROM (<34 Weeks Gestation) – Antibiotic Treatment to reduce risk of chorioamnionitis, prolong the latency period, and reduce neonatal morbidity. · Option 1: Ampicillin (2g IV q6h) and Erythromycin (250mg IV q6h) for 48 hours, followed by Amoxicillin (250mg PO, q8h) and Enteric-Coated Erythromycin Base (333mg PO q8h) for 5 days (Mercer protocol) · Option 2: Erythromycin (250mg PO q6h for 10 days) · Option 3: Clarithromycin or Azithromycin in appropriate doses (below) Do NOT administer amoxicillin with clavulanic acid (increased risk of necrotizing enterocolitis in the presence of PROM). Intrapartum Management:
Membrane Rupture or Onset of Active Labour: Administer to all women with (1) previous infant with invasive GBS disease, (2) GBS bacteriuria during current pregnancy, (3) positive screening culture within the past five weeks. If GBS status is unknown: Administer for (1) preterm labour (<37 weeks), (2) rupture of membranes for >18h, (3) maternal fever >38 degrees Celsius. NOT Indicated: (1) Planned Caesarean Section (CS) in the absence of labour or membrane rupture (regardless of GBS status) and (2) Negative vaginal and rectal GBS screening culture within five weeks. Preterm labour with intact membranes:
Prelabour rupture of membranes (PROM) and preterm PROM (PPROM):
|
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
First Stage |
|
|
Latent Phase Duration: Nulliparous: <20h Multiparous: <14h Clinical Features: Contractions:
Changes in Dilation:
|
Active Phase Duration: Nulliparous: 4-6h Multiparous: 2-3h Clinical Features: Contractions:
Changes in Dilation:
|
|
Clinical Features (Latent & Active Phases):
Overview of Physician Role:
|
|
|
Second Stage |
|
|
Duration: Nulliparous: <2h (3 with epidural) Multiparous: <1h (2 w/ epidural) Clinical Features:
Overview of Physician Role:
|
|
|
Third Stage |
|
|
Duration: 30 minutes Clinical Features:
Overview of Physician Role:
|
|
|
Fourth Stage |
|
|
1-2 hour postpartum period Clinical Features:
Overview of Physician Role:
|
|
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
1. Engagement, descent, and increased flexion (occur simultaneously)
2. Internal rotation: The fetal head rotates by 90° (two 45° steps) in the midpelvis, from a transverse to anterior-posterior position.
3. Extension: The fetal head, lying behind the symphysis pubis bone and the pelvic floor, acts upwards and forwards.
4. Restitution: The fetal head rotates 45° in the opposite direction as it passes through the pelvic outlet.
5. External rotation: The anterior shoulder rotates 45° anteriorly as it meets the maternal pelvic floor. This action is transmitted to the head which also rotates 45°, placing the head in its original transverse position.
6. Expulsion: Delivery of the head, anterior shoulder followed by the posterior shoulder, and the body.
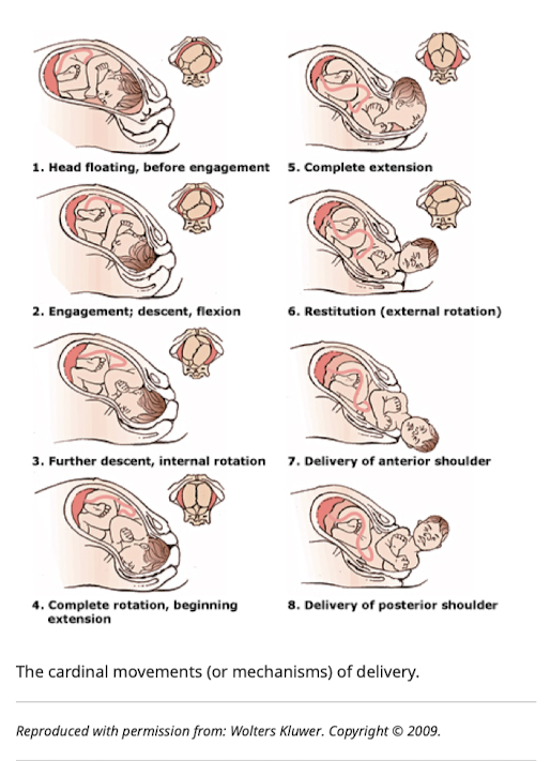
Funai, E. F., & Norwitz, E. R. (2022). Labor and delivery: Management of the normal second stage. In M. Prabhu (Ed.), UpToDate. Retrieved July 19, 2023, from https://www.uptodate.com/contents/labor-and-delivery-management-of-the-normal-second-stage
Proposed Methods:
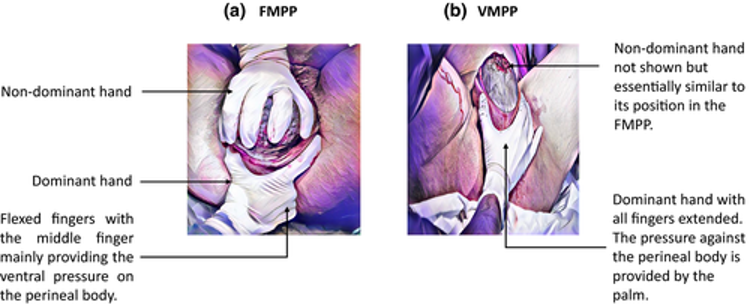
Kleprlikova, H, Kalis, V, Lucovnik, M, et al. Manual perineal protection: The know-how and the know-why. Acta Obstet Gynecol Scand. 2020; 99: 445– 450. https://doi.org/10.1111/aogs.13781
Brandt-Andrews Maneuver (preferred): an abdominal hand secures the uterine fundus to hold it in a fixed position and prevent uterine inversion while the other hand exerts sustained downward traction on the clamped umbilical cord.
Reference(s):
Anderson, Janice M, and Duncan Etches. 2007. Prevention and Management of Postpartum Hemorrhage. www.aafp.org/afp. (October 12, 2023).
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Created using information from: Simon LV, Hashmi MF, Bragg BN. APGAR Score. StatPearls. 2022 Feb. https://www.ncbi.nlm.nih.gov/books/NBK470569/
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
First Stage |
|
|
Latent Phase Duration: Nulliparous: <20h Multiparous: <14h Clinical Features: Contractions:
Changes in Dilation:
|
Active Phase Duration: Nulliparous: 4-6h Multiparous: 2-3h Clinical Features: Contractions:
Changes in Dilation:
|
|
Clinical Features (Latent & Active Phases):
Overview of Physician Role:
|
|
|
Second Stage |
|
|
Duration: Nulliparous: <2h (3 with epidural) Multiparous: <1h (2 w/ epidural) Clinical Features:
Overview of Physician Role:
|
|
|
Third Stage |
|
|
Duration: 30 minutes Clinical Features:
Overview of Physician Role:
|
|
|
Fourth Stage |
|
|
1-2 hour postpartum period Clinical Features:
Overview of Physician Role:
|
|
Brandt-Andrews Maneuver (preferred): an abdominal hand secures the uterine fundus to hold it in a fixed position and prevent uterine inversion while the other hand exerts sustained downward traction on the clamped umbilical cord.
Reference(s):
Anderson, Janice M, and Duncan Etches. 2007. Prevention and Management of Postpartum Hemorrhage. www.aafp.org/afp. (October 12, 2023).
|
Definition |
|
Lack of placental expulsion within 30 minutes of delivery. This time period can be extended to 90 to 120 minutes in the absence of hemorrhage for births in the second trimester and third stages of labor managed without oxytocin. In 80% of term births, the placenta is expelled within 30 minutes and in 98% within 1 hour. |
|
Etiology & Clinical Features |
|
There are 3 types of retained placenta:
|
|
Risk Factors |
|
|
Complications |
|
Most common complications include postpartum hemorrhage and postpartum endometritis. Uterine inversion is less common. Fatality is quite rare in high-resource settings. |
|
Management |
|
Indications for Intervention:
Management:
|
|
Reference(s) Erickson, A. & Parker, J. (Eds.). (2023). Toronto Notes 2023: Comprehensive Medical Reference and a Review for MCCQE. Toronto Notes for Medical Students Inc. Weeks, A. (2023). Retained placenta after vaginal birth. In Barss V (Ed.), UpToDate. Retrieved August 9, 2023 from https://www.uptodate.com/contents/retained-placenta-after-vaginal-birth?search=retained%20placenta%20after%20vaginal%20birth&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 |
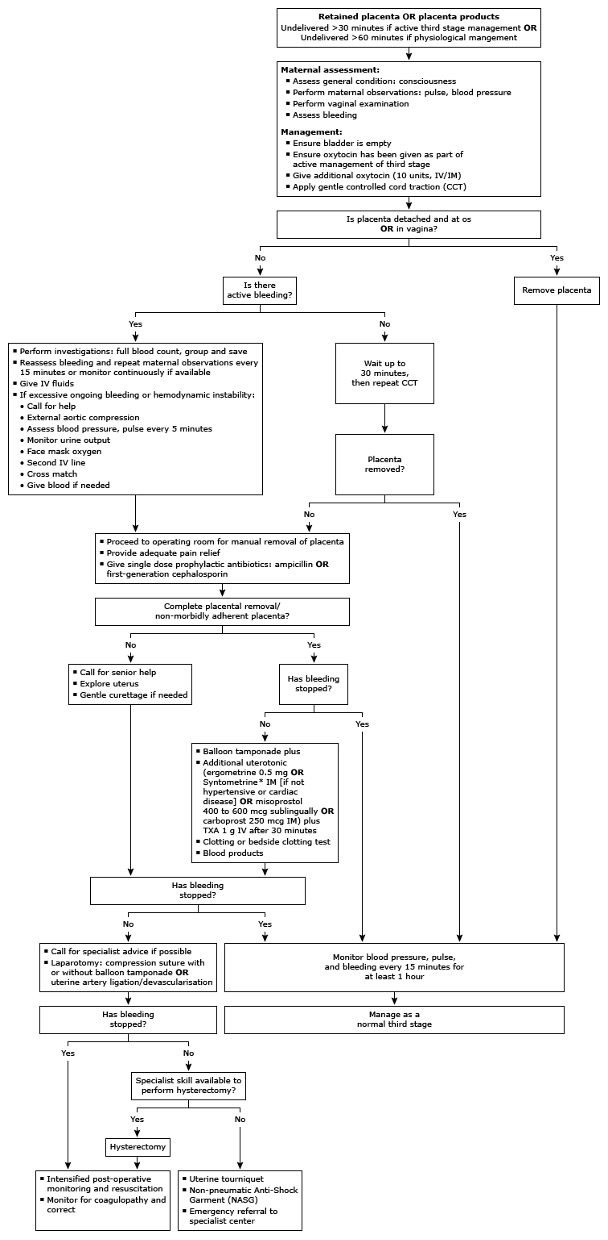
IV: intravenous
IM: intramuscular
TXA: tranexamic acid
CCT: controlled cord traction
group and save: this is another term for type and screen or type and hold.
*Generic name ergometrine-oxytocin.
Reference(s):
Weeks, A. (2023). Retained placenta after vaginal birth. In Barss V (Ed.), UpToDate. Retrieved August 9, 2023 from https://www.uptodate.com/contents/retained-placenta-after-vaginal-birth?search=retained%20placenta%20after%20vaginal%20birth&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
|
First Stage |
|
|
Latent Phase Duration: Nulliparous: <20h Multiparous: <14h Clinical Features: Contractions:
Changes in Dilation:
|
Active Phase Duration: Nulliparous: 4-6h Multiparous: 2-3h Clinical Features: Contractions:
Changes in Dilation:
|
|
Clinical Features (Latent & Active Phases):
Overview of Physician Role:
|
|
|
Second Stage |
|
|
Duration: Nulliparous: <2h (3 with epidural) Multiparous: <1h (2 w/ epidural) Clinical Features:
Overview of Physician Role:
|
|
|
Third Stage |
|
|
Duration: 30 minutes Clinical Features:
Overview of Physician Role:
|
|
|
Fourth Stage |
|
|
1-2 hour postpartum period Clinical Features:
Overview of Physician Role:
|
|
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Brandt-Andrews Maneuver (preferred): an abdominal hand secures the uterine fundus to hold it in a fixed position and prevent uterine inversion while the other hand exerts sustained downward traction on the clamped umbilical cord.
Reference(s):
Anderson, Janice M, and Duncan Etches. 2007. Prevention and Management of Postpartum Hemorrhage. www.aafp.org/afp. (October 12, 2023).
|
Definition |
|
Lack of placental expulsion within 30 minutes of delivery. This time period can be extended to 90 to 120 minutes in the absence of hemorrhage for births in the second trimester and third stages of labor managed without oxytocin. In 80% of term births, the placenta is expelled within 30 minutes and in 98% within 1 hour. |
|
Etiology & Clinical Features |
|
There are 3 types of retained placenta:
|
|
Risk Factors |
|
|
Complications |
|
Most common complications include postpartum hemorrhage and postpartum endometritis. Uterine inversion is less common. Fatality is quite rare in high-resource settings. |
|
Management |
|
Indications for Intervention:
Management:
|
|
Reference(s) Erickson, A. & Parker, J. (Eds.). (2023). Toronto Notes 2023: Comprehensive Medical Reference and a Review for MCCQE. Toronto Notes for Medical Students Inc. Weeks, A. (2023). Retained placenta after vaginal birth. In Barss V (Ed.), UpToDate. Retrieved August 9, 2023 from https://www.uptodate.com/contents/retained-placenta-after-vaginal-birth?search=retained%20placenta%20after%20vaginal%20birth&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 |
IV: intravenous
IM: intramuscular
TXA: tranexamic acid
CCT: controlled cord traction
group and save: this is another term for type and screen or type and hold.
*Generic name ergometrine-oxytocin.
Reference(s):
Weeks, A. (2023). Retained placenta after vaginal birth. In Barss V (Ed.), UpToDate. Retrieved August 9, 2023 from https://www.uptodate.com/contents/retained-placenta-after-vaginal-birth?search=retained%20placenta%20after%20vaginal%20birth&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
| Signs of Placental Separation | |
|
1. Gush of blood |
|
| Active Management | |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
| Signs of Placental Separation | |
|
1. Gush of blood |
|
| Active Management | |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Equipment Recommendations:
Monitoring:
Antiemetics
Dosing
Procedural Sedation & Analgesia Medications & Dosing

Adapted from Frank, R. L. (2023). Procedural sedation in adults: Medication selection, dosing, and discharge criteria. M Ganetsky (Ed.) UpToDate. Retreived August 23, 2023 from https://www.uptodate.com/contents/procedural-sedation-in-adults-medication-selection-dosing-and-discharge-criteria?search=procedural%20sedation%20drugs&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H3175829286
Provincial Massive Hemorrhage Protocol: https://transfusionontario.org/wp-content/uploads/2021/10/Recommendation-Statements_April-2021-1.pdf
Ontario Regional Blood Coordinating Network. Ontario MHP: Guidance for small/remote hospitals. https://youtu.be/ofvNsScQ58M?feature=shared
Refractory Hemorrhage Caution:
E.g., for hemorrhagic shock with ongoing bleeding, crystalloid administration may dilute the coagulation factors and RBC concentration. Beginning resuscitation with crystalloid early may promote volume overload.
Minimum Laboratory Protocol Resuscitation Targets for Transfusion:
Provincial Massive Hemorrhage Protocol: https://transfusionontario.org/wp-content/uploads/2021/10/Recommendation-Statements_April-2021-1.pdf
Ontario Regional Blood Coordinating Network. Ontario MHP: Guidance for small/remote hospitals. https://youtu.be/ofvNsScQ58M?feature=shared
Refractory Hemorrhage Caution:
E.g., for hemorrhagic shock with ongoing bleeding, crystalloid administration may dilute the coagulation factors and RBC concentration. Beginning resuscitation with crystalloid early may promote volume overload.
Minimum Laboratory Protocol Resuscitation Targets for Transfusion:
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
|
First Stage |
|
|
Latent Phase Duration: Nulliparous: <20h Multiparous: <14h Clinical Features: Contractions:
Changes in Dilation:
|
Active Phase Duration: Nulliparous: 4-6h Multiparous: 2-3h Clinical Features: Contractions:
Changes in Dilation:
|
|
Clinical Features (Latent & Active Phases):
Overview of Physician Role:
|
|
|
Second Stage |
|
|
Duration: Nulliparous: <2h (3 with epidural) Multiparous: <1h (2 w/ epidural) Clinical Features:
Overview of Physician Role:
|
|
|
Third Stage |
|
|
Duration: 30 minutes Clinical Features:
Overview of Physician Role:
|
|
|
Fourth Stage |
|
|
1-2 hour postpartum period Clinical Features:
Overview of Physician Role:
|
|
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Reference(s):
Argani, A. H., & Satin, A. J. (2022). Occiput Posteror Position. In Barss V (Ed.), UpToDate. Retrieved Aug 20, 2023, from https://www.uptodate.com/contents/occiput-posterior-position?search=occiput%20posterior%20position&source=search_result&selectedTitle=1~13&usage_type=default&display_rank=1#references

Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
|
|
|
|
|
→ total # of pregnancies
|
E.g., Patient has been pregnant 4 times. The first one ended in a miscarriage at 10 weeks, the second child was born healthy at 38 weeks, the third was carried to 23 weeks but was born stillborn and she is currently 35 weeks gestation with the fourth pregnancy.
This can be described as: G4P2 in GxPx format or G4T1P1A1L1 in the GTPAL format.
Leopold Maneuvers: Systematic abdominal palpation maneuvers performed after 30-32 weeks gestation. They are used to determine the presentation, position, and engagement of the fetus in utero.
from Toronto Notes 2022
Fetal Orientation:
|
1. Fetal Lie: Relation of fetal long axis to long maternal uterus |
|
|
|
|
2. Presentation: The part of the fetus that overlies pelvic inlet (separation between abdominal & pelvic organs - borders include sacral promontory & pubic symphysis) |
|
|
Cephalic (head down in pelvic inlet) - most common Compound (more than one part presenting - e.g., cephalic or breech + extremity |
|
|
3. Fetal Position: Relationship to maternal pelvis |
|
|
Occiput Anterior (OA) - fetal occiput (posterior head) towards pubic symphysis (face down) |
|
|
4. Fetal Attitude: How much the fetal head flexes/extends during cephalic presentation |
|
|
Vertex - maximum flexion (most common) *spontaneous vaginal delivery possible in all attitudes |
|
|
5. Fetal Station: Measurement (in cm) of where the presenting part of the fetus is located in the pelvis, in relation to ischial spine |
|
|
Negative (-) = above ischial spine |
|
|
6. Synclitism: Parallelism between pelvic plane and plane of fetal head |
|
|
Synclitism - posture in which the 2 parietal bones are at the same level |
Retrieved July 2, 2023 from: https://www.parents.com/pregnancy/giving-birth/labor-and-delivery/cervix-dilation-chart-pictures-that-explain-the-stages-of-labor/
Retrieved July 27, 2023 from: https://www.instagram.com/p/CHJCbAhgdIu/?utm_source=ig_web_button_share_sheet
Retrieved July 27, 2023 from: https://www.youtube.com/watch?v=x17vY7_3M2M
Adapted September 12, 2023 from https://www.medicalnewstoday.com/articles/326380
|
First Stage |
|
|
Latent Phase Duration: Nulliparous: <20h Multiparous: <14h Clinical Features: Contractions:
Changes in Dilation:
|
Active Phase Duration: Nulliparous: 4-6h Multiparous: 2-3h Clinical Features: Contractions:
Changes in Dilation:
|
|
Clinical Features (Latent & Active Phases):
Overview of Physician Role:
|
|
|
Second Stage |
|
|
Duration: Nulliparous: <2h (3 with epidural) Multiparous: <1h (2 w/ epidural) Clinical Features:
Overview of Physician Role:
|
|
|
Third Stage |
|
|
Duration: 30 minutes Clinical Features:
Overview of Physician Role:
|
|
|
Fourth Stage |
|
|
1-2 hour postpartum period Clinical Features:
Overview of Physician Role:
|
|
|
|
|||||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|||||||||||
|
|
|
|
|
||||||||
|
|
|
|
Normal (palpation): soft between contractions for at least 30s to allow for placental perfusion
|
||||||||
|
|
|||||||||||
|
|
|||||||||||
Important Notes Regarding Pharmacological use in Labour:
Options for Pharmacological Pain Management in Labour (see dosing information below):
Suggested Opioid use in labour:
|
Stage of Labour |
Nulliparous |
Parous |
|
Latent Stage: |
IM/SC Morphine |
IM/SC Morphine |
|
Early Active Stage: |
IM/SC or IV Morphine |
IV Morphine or Fentanyl |
|
Late Active Stage: |
IV Morphine or Fentanyl |
IV Fentanyl |
|
Second Stage: |
IV Fentanyl |
IV Fentanyl |
Reference(s):
Grant G. (2022). Pharmacologic management of pain during labor and delivery. In Crowley M (Ed.), UpToDate. Retrieved Jul 2, 2023, from https://www.uptodate.com/contents/pharmacologic-management-of-pain-during-labor-and-delivery
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
1. Engagement, descent, and increased flexion (occur simultaneously)
2. Internal rotation: The fetal head rotates by 90° (two 45° steps) in the midpelvis, from a transverse to anterior-posterior position.
3. Extension: The fetal head, lying behind the symphysis pubis bone and the pelvic floor, acts upwards and forwards.
4. Restitution: The fetal head rotates 45° in the opposite direction as it passes through the pelvic outlet.
5. External rotation: The anterior shoulder rotates 45° anteriorly as it meets the maternal pelvic floor. This action is transmitted to the head which also rotates 45°, placing the head in its original transverse position.
6. Expulsion: Delivery of the head, anterior shoulder followed by the posterior shoulder, and the body.
Funai, E. F., & Norwitz, E. R. (2022). Labor and delivery: Management of the normal second stage. In M. Prabhu (Ed.), UpToDate. Retrieved July 19, 2023, from https://www.uptodate.com/contents/labor-and-delivery-management-of-the-normal-second-stage
Proposed Methods:
Kleprlikova, H, Kalis, V, Lucovnik, M, et al. Manual perineal protection: The know-how and the know-why. Acta Obstet Gynecol Scand. 2020; 99: 445– 450. https://doi.org/10.1111/aogs.13781
Delivery with Nuchal Cord
Management
Retrieved Aug 1, 2023 from https://www.youtube.com/watch?v=6nZtMT4YhnA
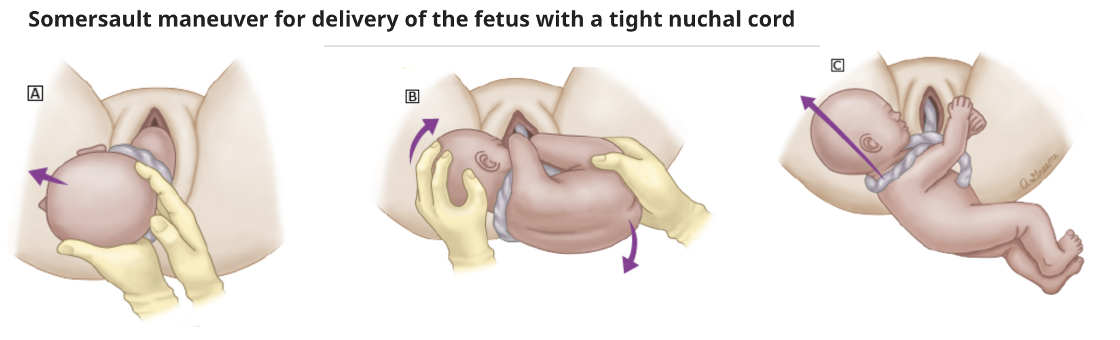
Schaffer, L. & Zimmermann, R. (2022). Nuchal Cord. In Chakrabarti A (Ed.), UpToDate. Retrieved Aug 1, 2023, from https://www.uptodate.com/contents/nuchal-cord?search=nuchal%20cord&source=search_result&selectedTitle=1~14&usage_type=default&display_rank=1
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Created using information from: Simon LV, Hashmi MF, Bragg BN. APGAR Score. StatPearls. 2022 Feb. https://www.ncbi.nlm.nih.gov/books/NBK470569/
| Signs of Placental Separation | |
|
1. Gush of blood |
|
| Active Management | |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
Reference(s):
Society of Obstetricians and Gynecologists of Canada. ALARM Manual, 28th Ed. 2022.
Clinical Pearls:
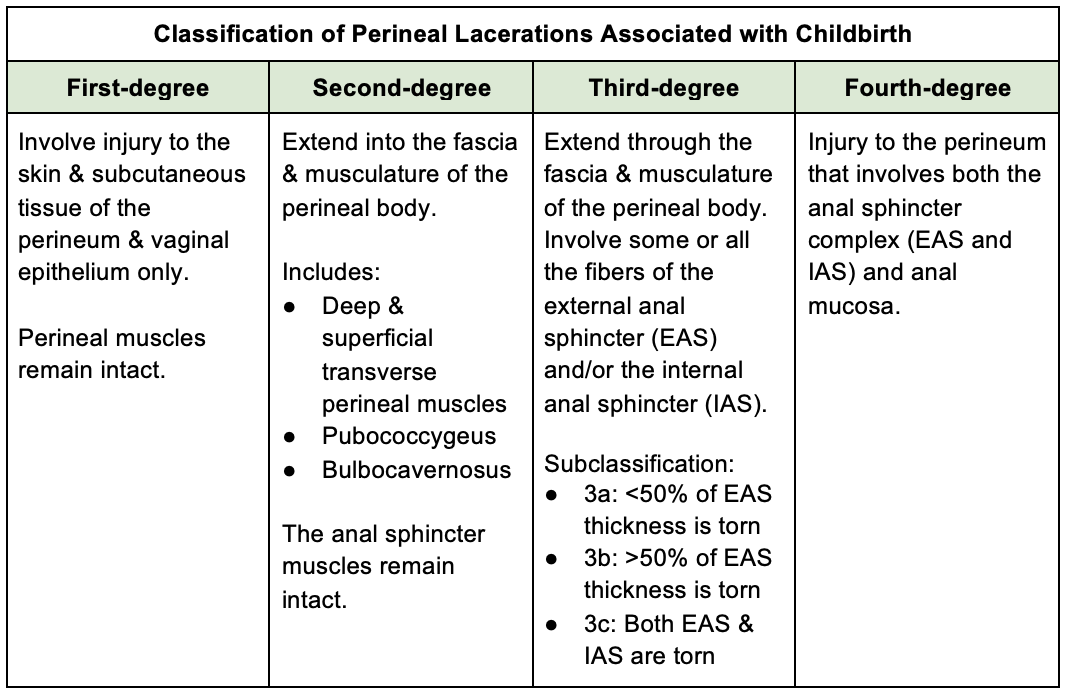
Preparation
Anesthesia
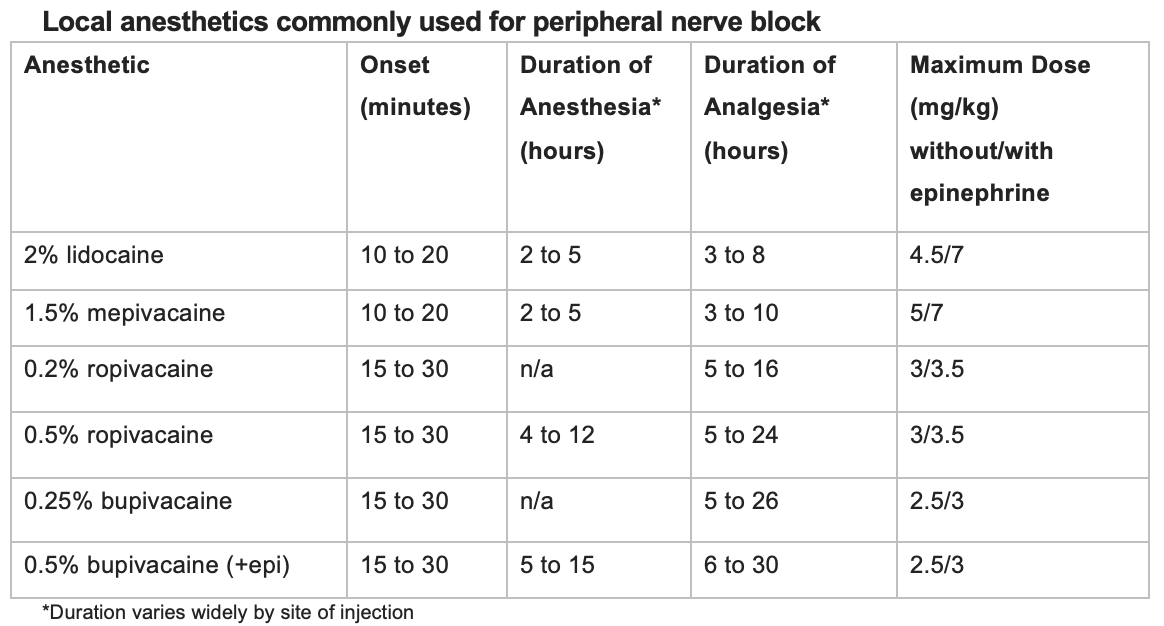
Vidaeff, A. C. (2023). Pudendal and paracervical block. In Eckler K (Ed.), UpToDate. Retrieved August 2, 2023 From https://www.uptodate.com/contents/pudendal-and-paracervical-block?search=controlled%20cord%20traction%20&topicRef=5399&source=see_link#H3
Pudendal Block
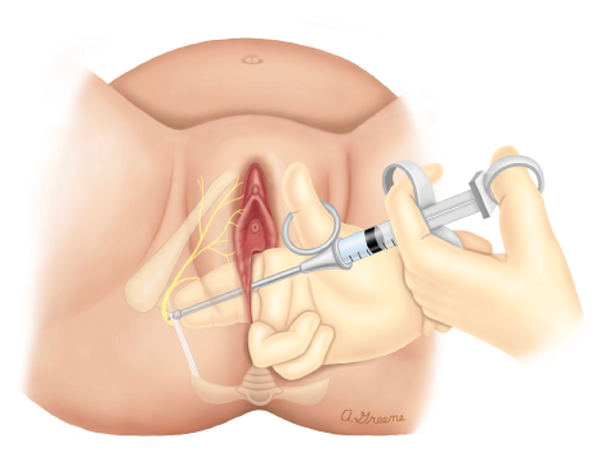
Vidaeff, A. C. (2023). Pudendal and paracervical block. In Eckler K (Ed.), UpToDate. Retrieved August 2, 2023 From https://www.uptodate.com/contents/pudendal-and-paracervical-block?search=controlled%20cord%20traction%20&topicRef=5399&source=see_link#H3
See https://www.youtube.com/watch?v=gWWXzJmT7cg for explanation of injection site.
Choice of Suture
Repair Technique
Third- & Fourth-degree tears can be difficult and should be repaired first. This type of perineal trauma should ideally be repaired in the operating room with regional or general anesthetic and appropriate lighting. Transfer to appropriate medical centre.
Repair of First- and Second-degree Perineal Trauma:
Step 1 – Suturing the vaginal wall
Step 2 – Suturing the perineal muscle layer
Step 3 – Suturing the skin layer
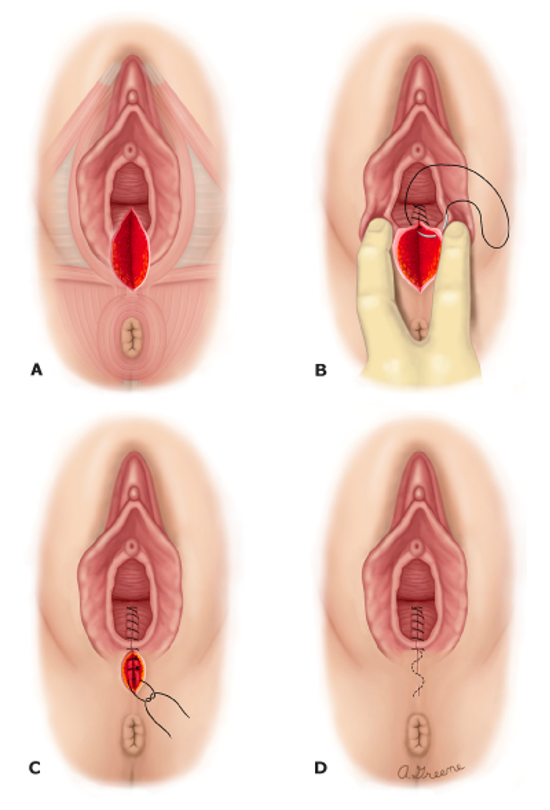
(A) Second-degree median episiotomy
(B) The vaginal epithelium to just outside the hymenal ring is reapproximated first.
(C) The perineal body and bulbocavernosus muscle are then reapproximated with intermittent or continuous sutures. The perineal skin can be reapproximated with a continuous running subcuticular suture.
(D) Completed repair.
Toglia, M. R. (2022). Repair of perineal lacerations associated with childbirth. In Eckler K (Ed.), UpToDate. Retrieved August 2, 2023, from https://www.uptodate.com/contents/repair-of-perineal-lacerations-associated-with-childbirth?search=controlled%20cord%20traction%20&topicRef=134954&source=see_link#H1697103
Reference(s)
Maternity Services. (2019). Perineal Assessment and Repair Following childbirth: Guideline for Midwives, Aneurin Bevan University Health Board. Retrieved July 31, 2023, from https://wisdom.nhs.wales/health-board-guidelines/aneurin-bevan-file/perineal-assessment-and-repair-following-childbirth-guideline-for-midwives-aneurin-bevan-2016-pdf/
The Royal Women’s Hospital. (2020). Guideline: Perineal Trauma Assessment, Repair and Safe Practice. The Royal Women’s Hospital. Retrieved August 1, 2023 from https://thewomens.r.worldssl.net/images/uploads/downloadable-records/clinical-guidelines/perineal-trauma-assessment-repair-and-safe-practice_280720.pdf
Toglia, M. R. (2022). Repair of perineal lacerations associated with childbirth. In Eckler K (Ed.), UpToDate. Retrieved August 2, 2023, from https://www.uptodate.com/contents/repair-of-perineal-lacerations-associated-with-childbirth?search=controlled%20cord%20traction%20&topicRef=134954&source=see_link#H1697103
Vidaeff, A. C. (2023). Pudendal and paracervical block. In Eckler K (Ed.), UpToDate. Retrieved August 2, 2023 From https://www.uptodate.com/contents/pudendal-and-paracervical-block?search=controlled%20cord%20traction%20&topicRef=5399&source=see_link#H3
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Created using information from: Simon LV, Hashmi MF, Bragg BN. APGAR Score. StatPearls. 2022 Feb. https://www.ncbi.nlm.nih.gov/books/NBK470569/
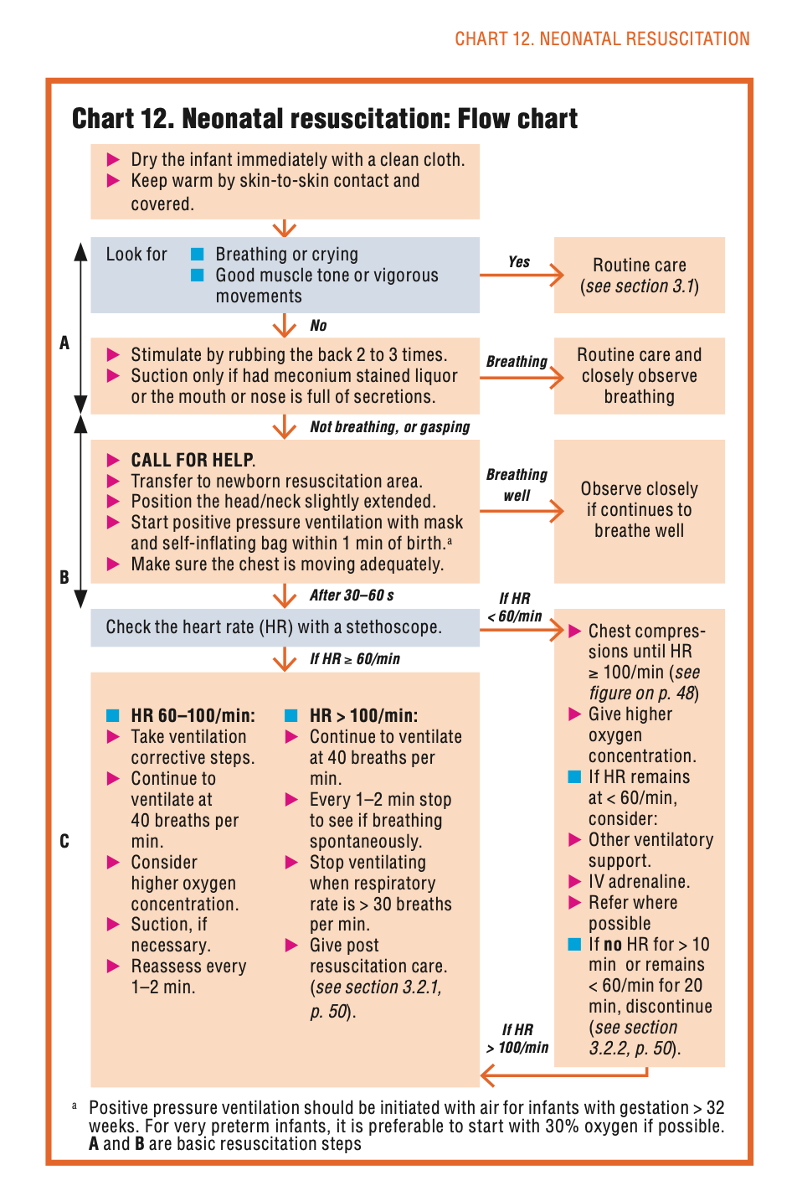



bpm: beats per minute; PPV: positive pressure ventilation; CPAP: continuous positive airway pressure; HR: heart rate; ETT: endotracheal tube; GA: gestational age.
*If there is no labored breathing or persistent cyanosis, the neonate stays with the mother for ongoing evaluation. Refer to UpToDate's topics on initial management of newborn infants for additional details.
UpToDate: Neonatal resuscitation in the delivery room.

UpToDate: Neonatal resuscitation in the delivery room.

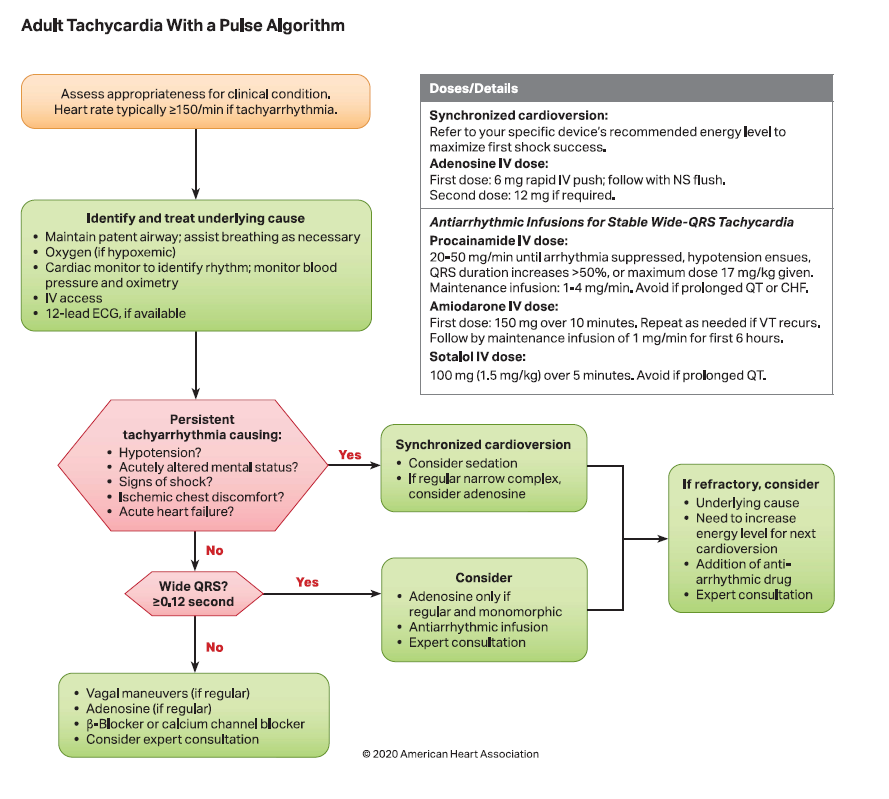
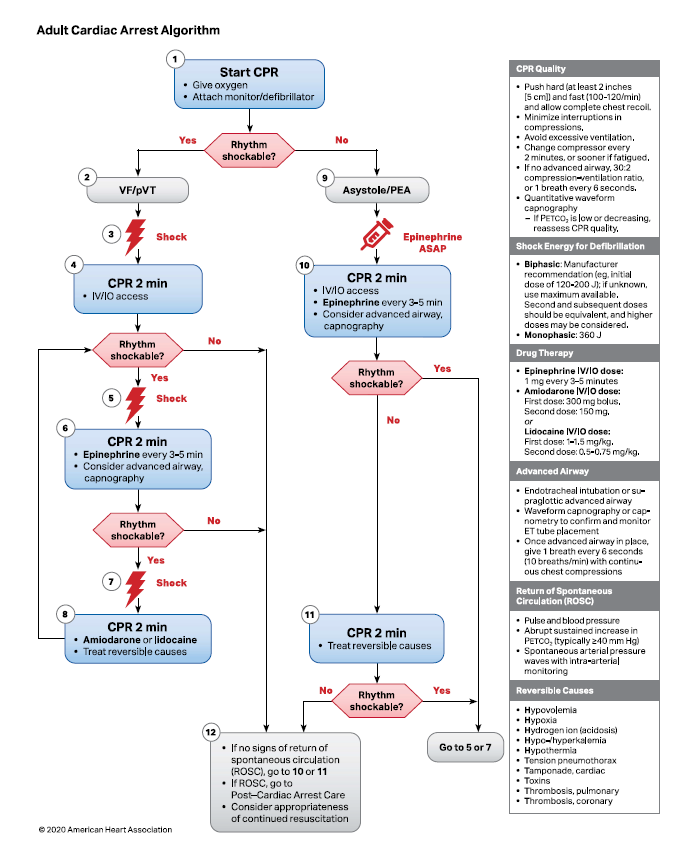
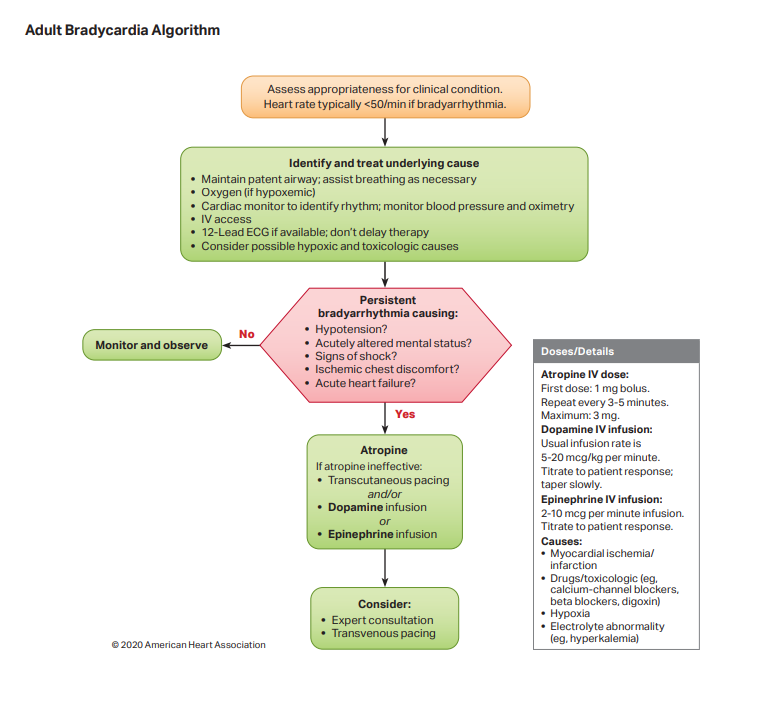
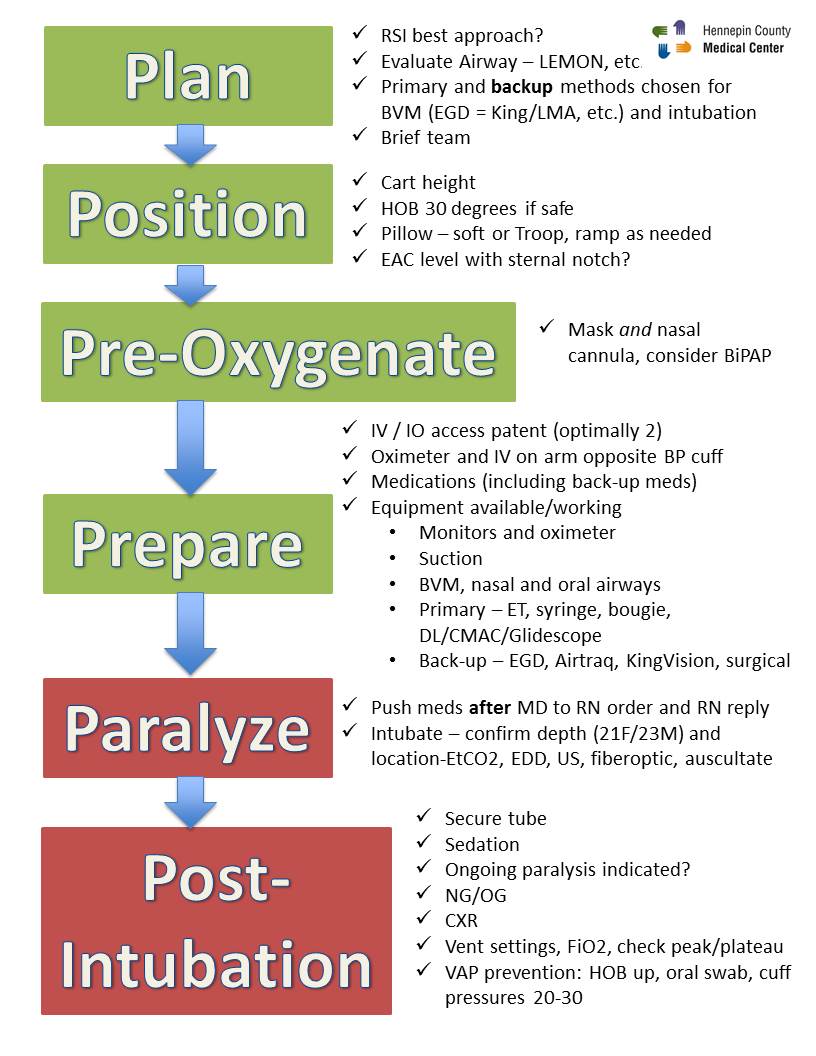

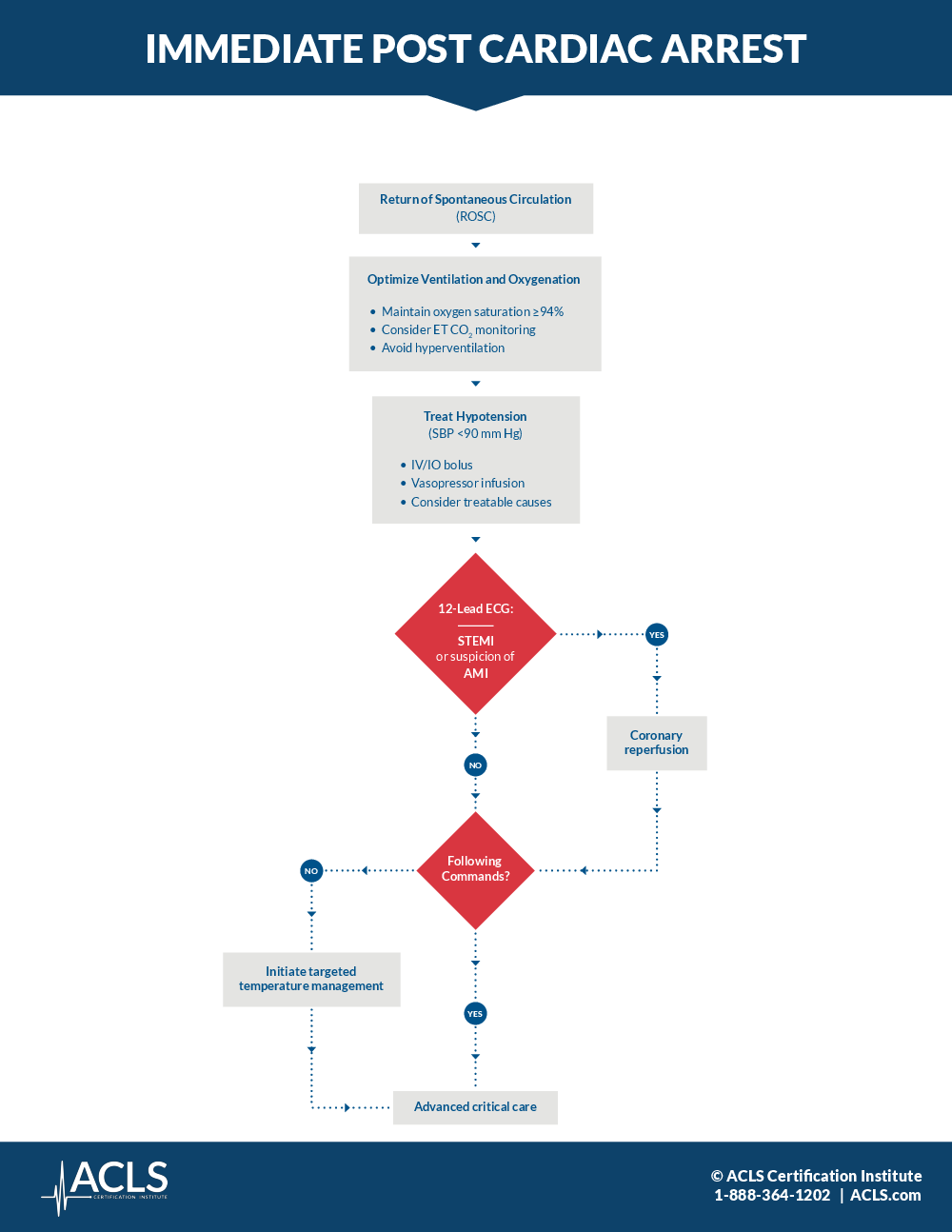
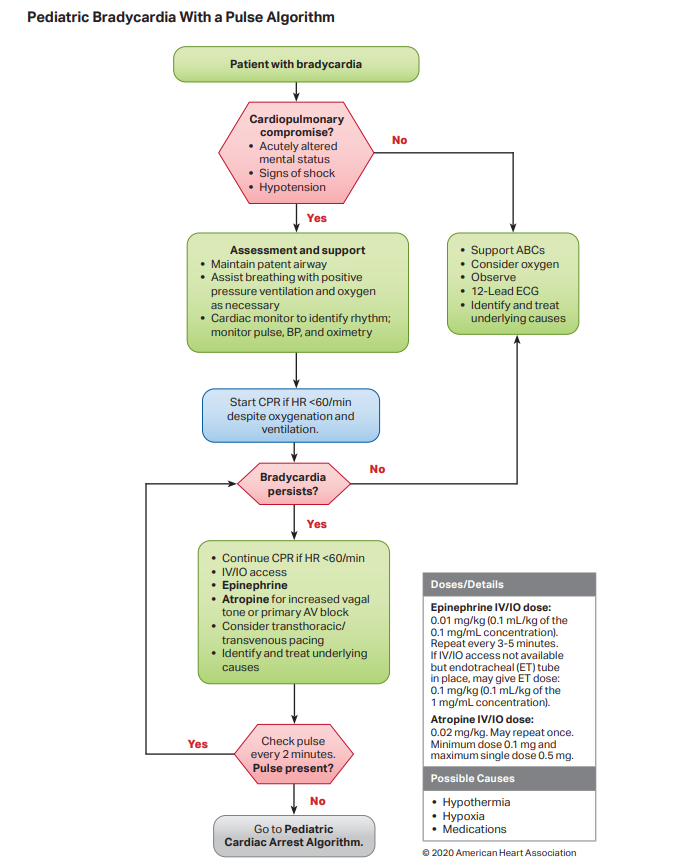
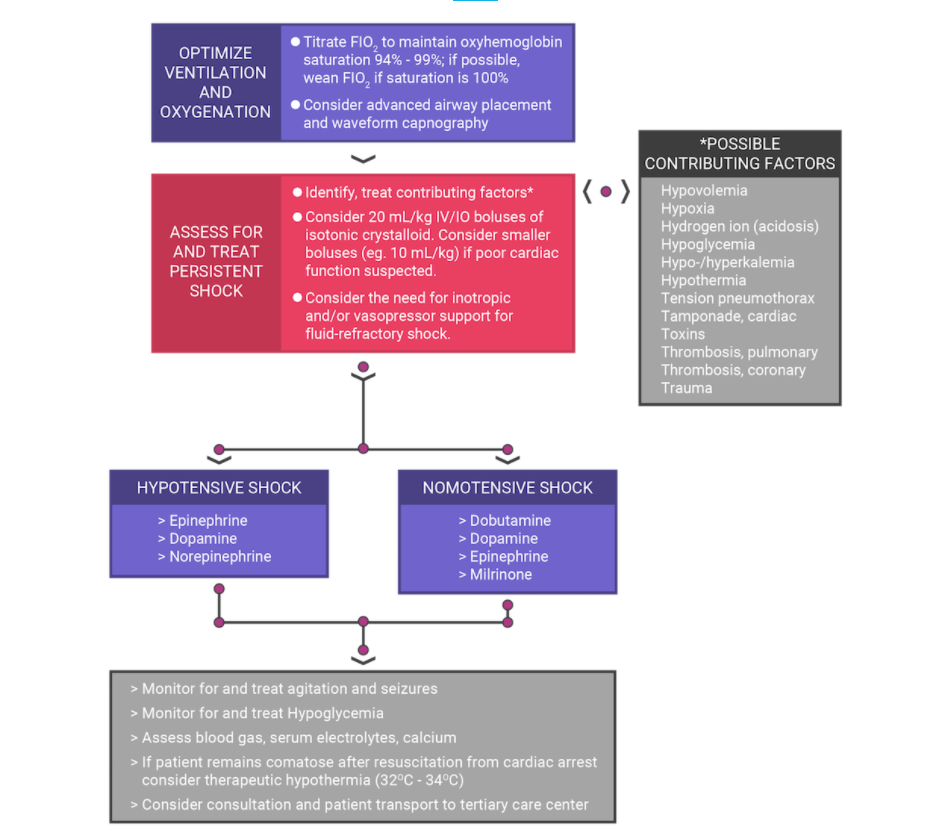
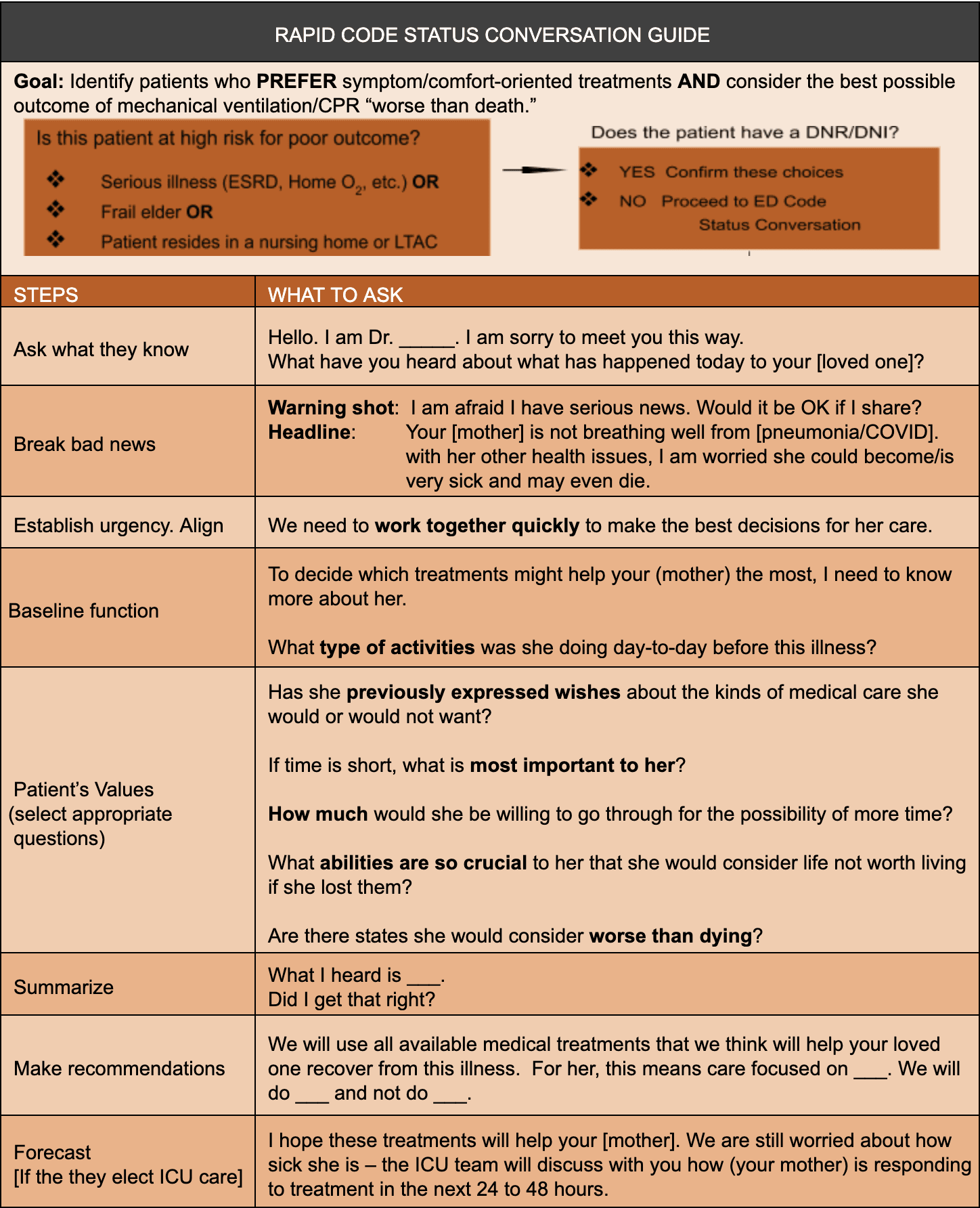
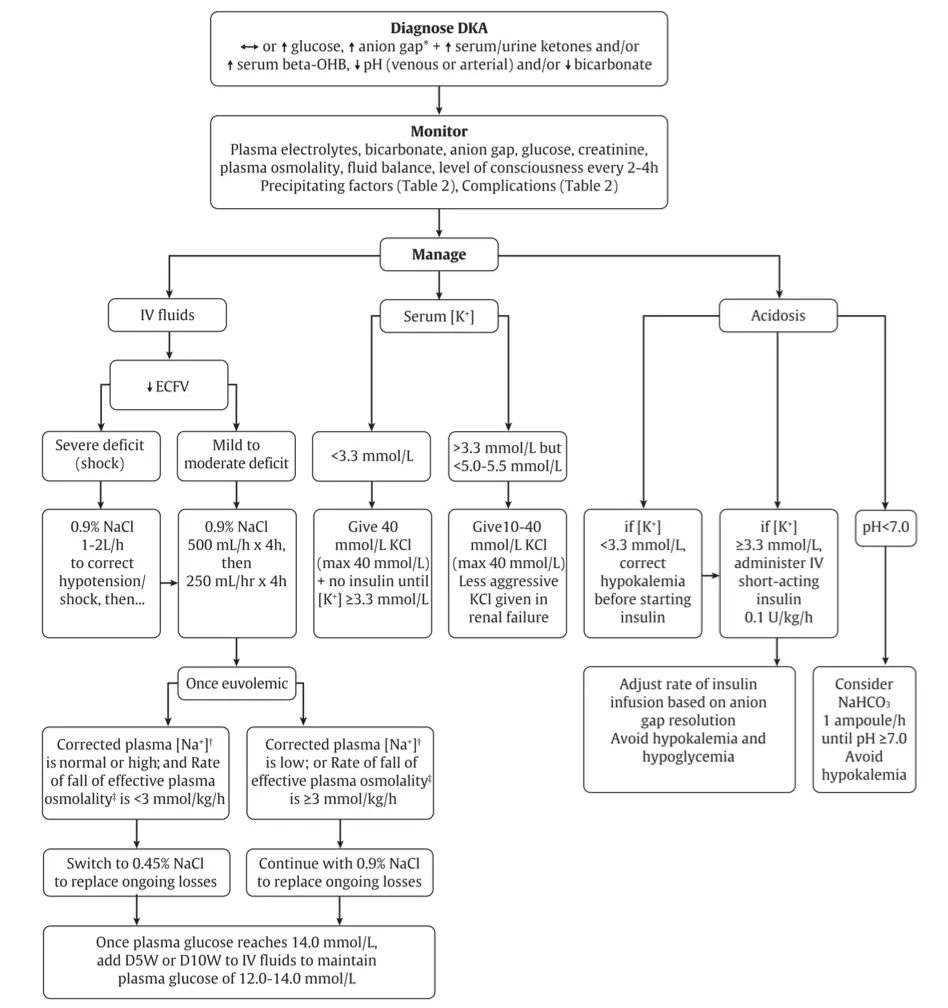

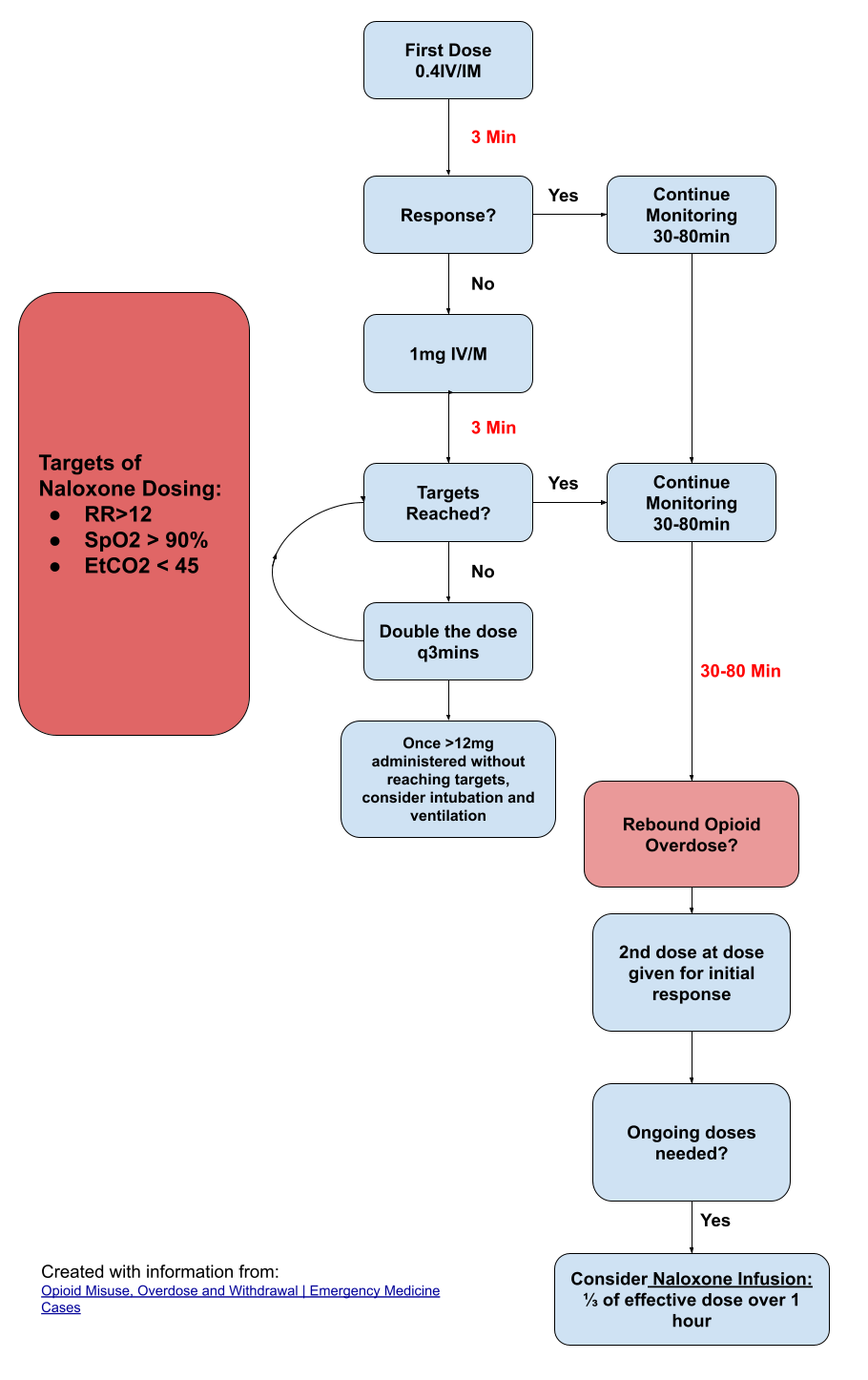

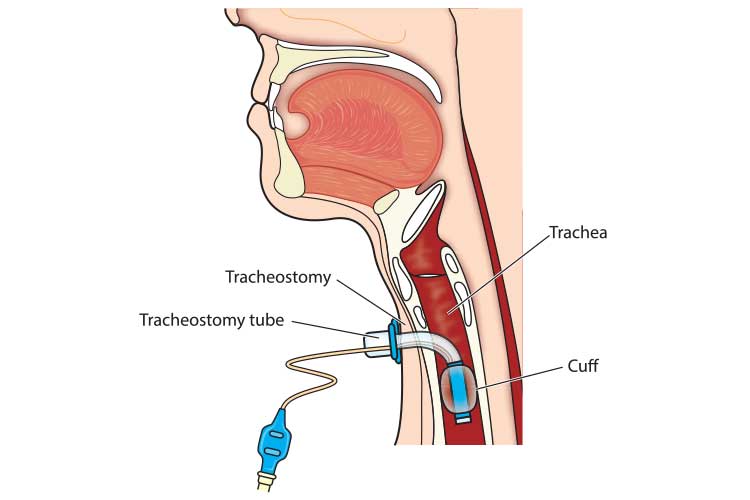


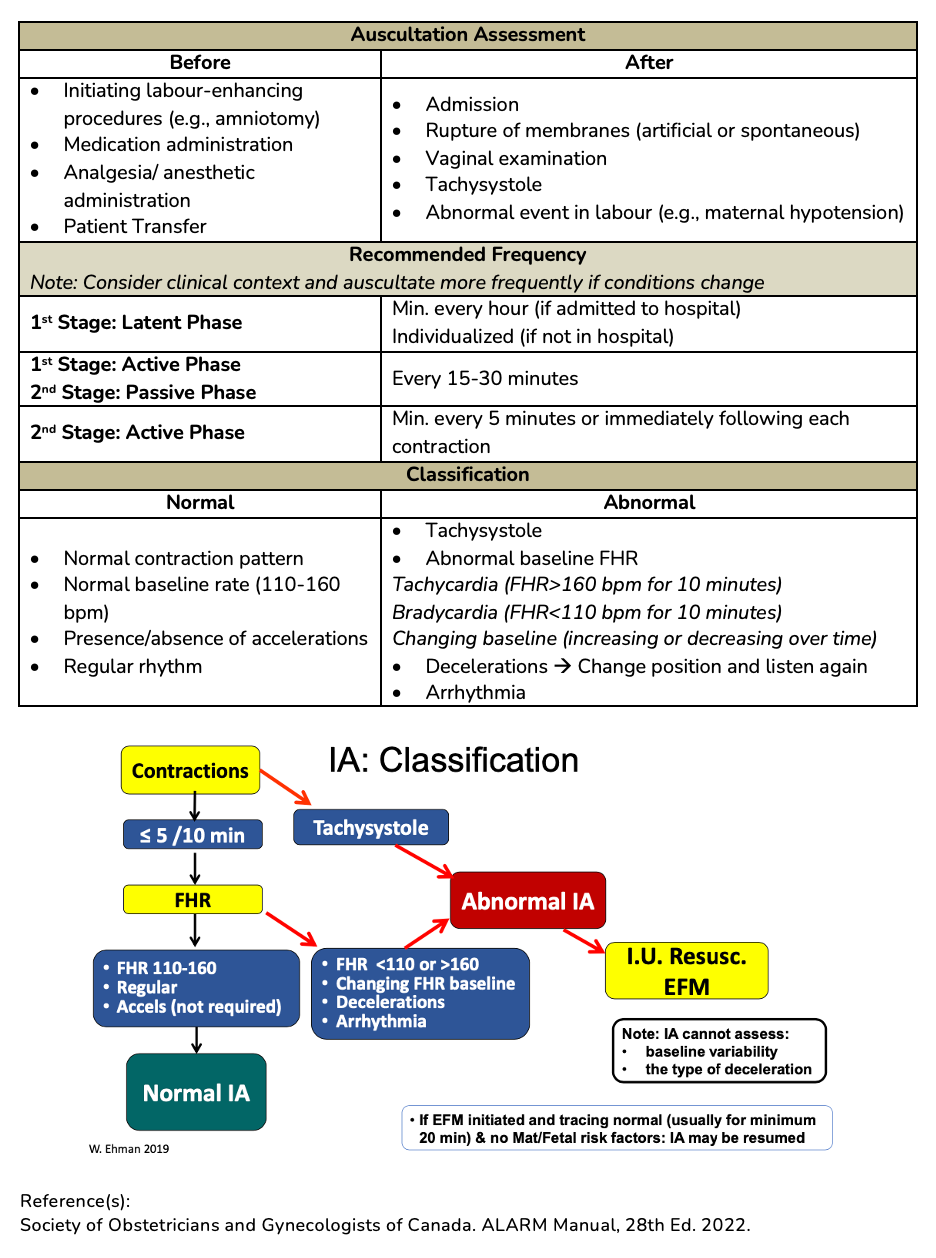
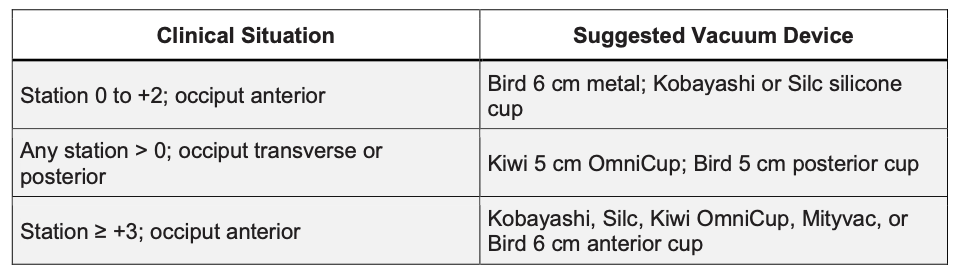
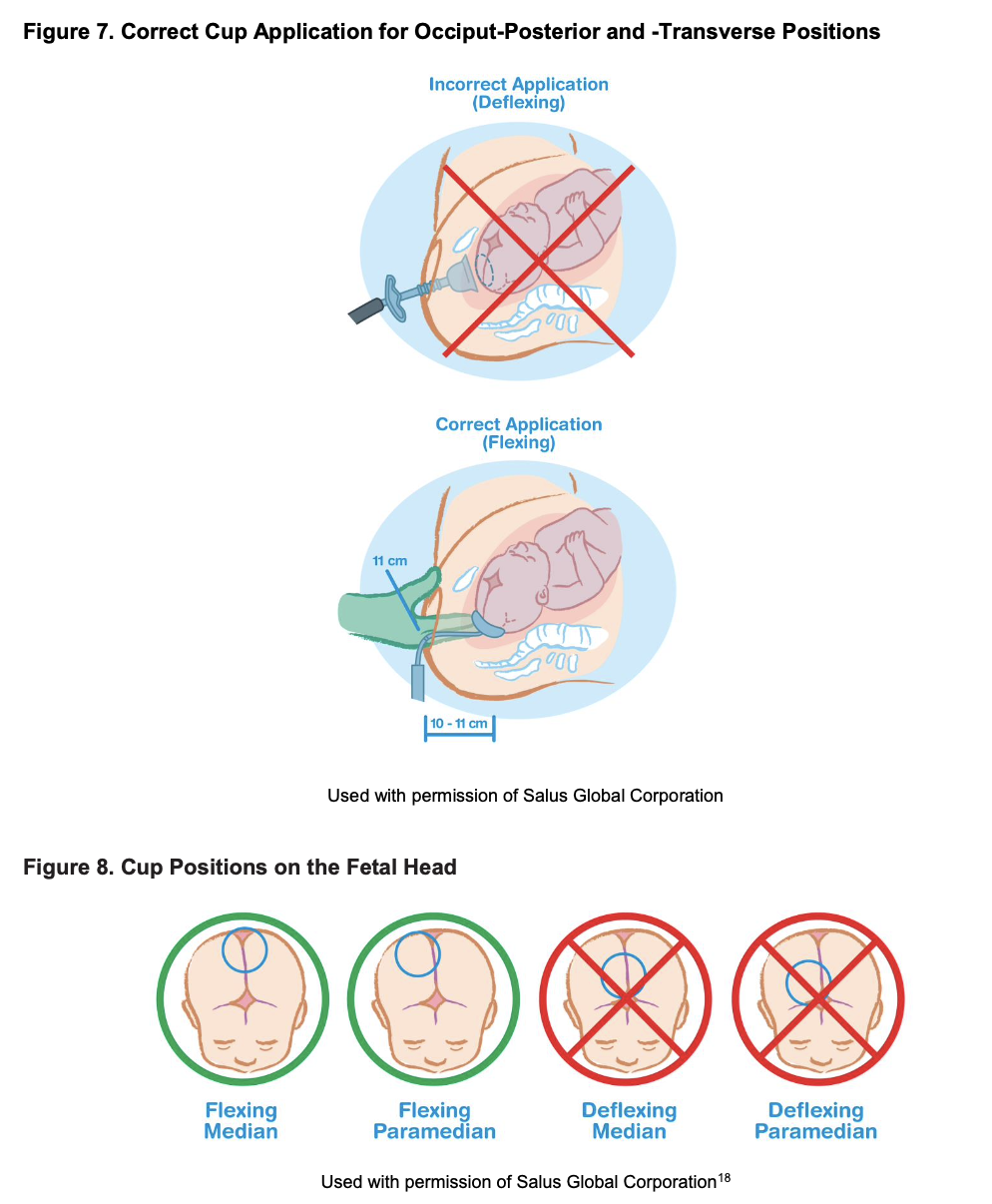

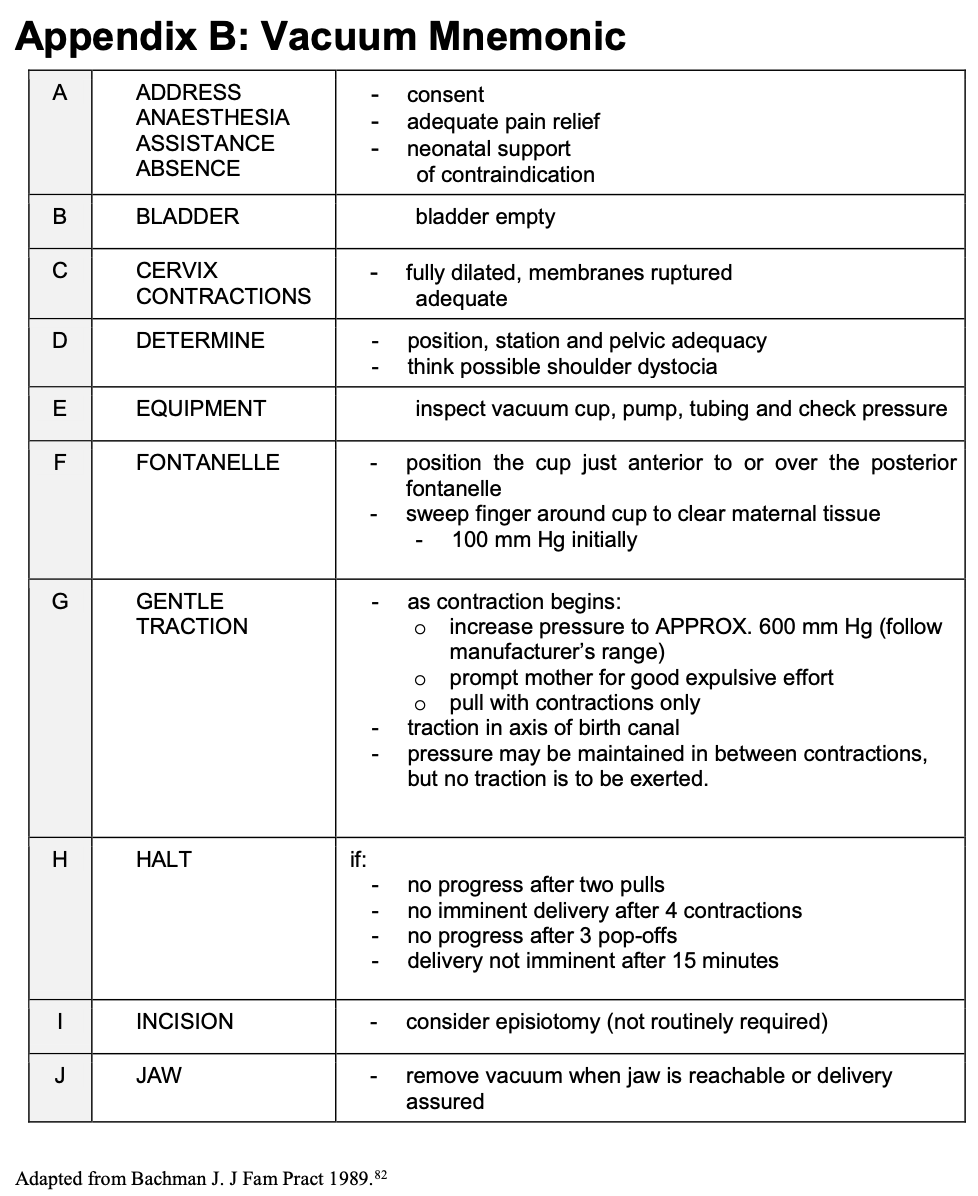
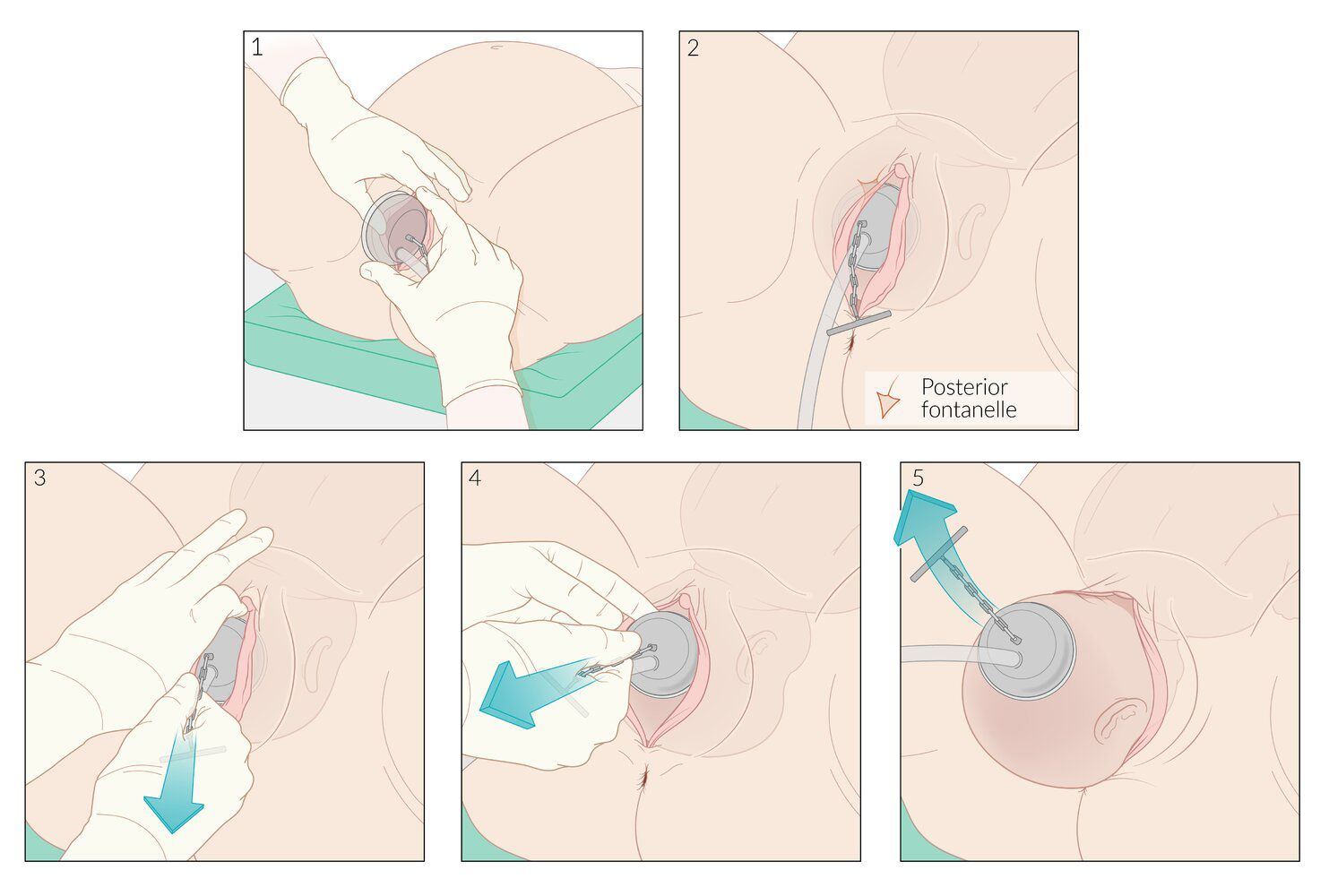
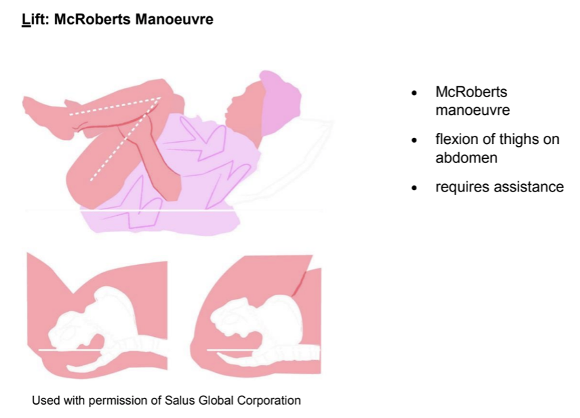
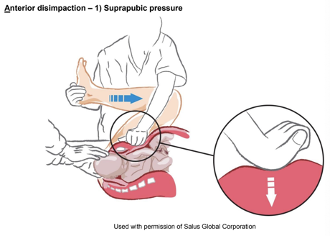
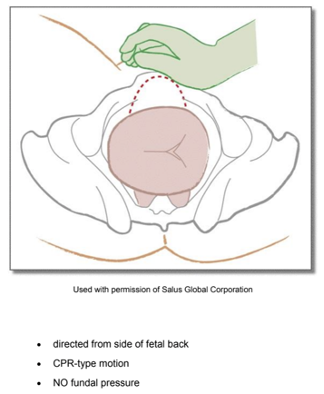


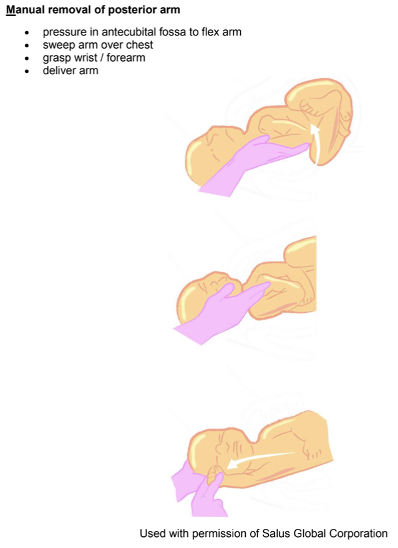
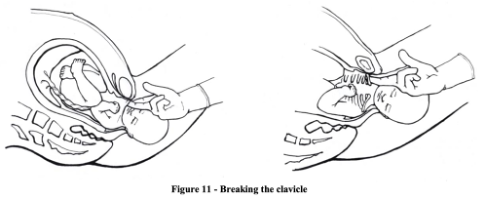


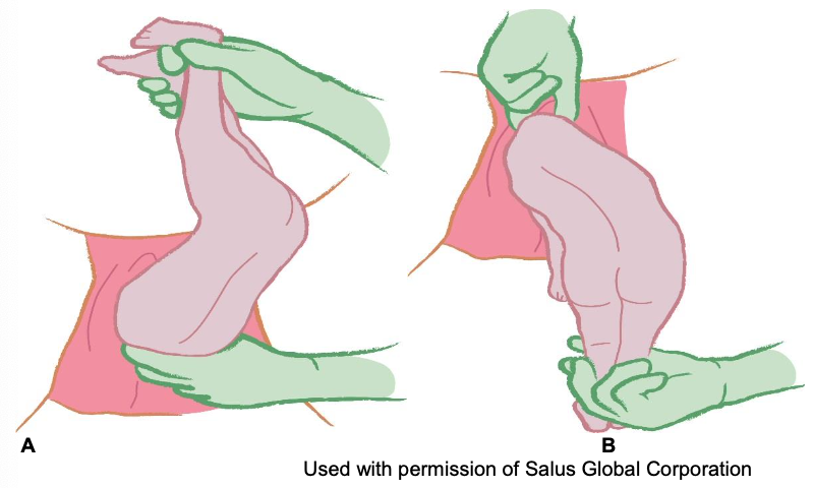
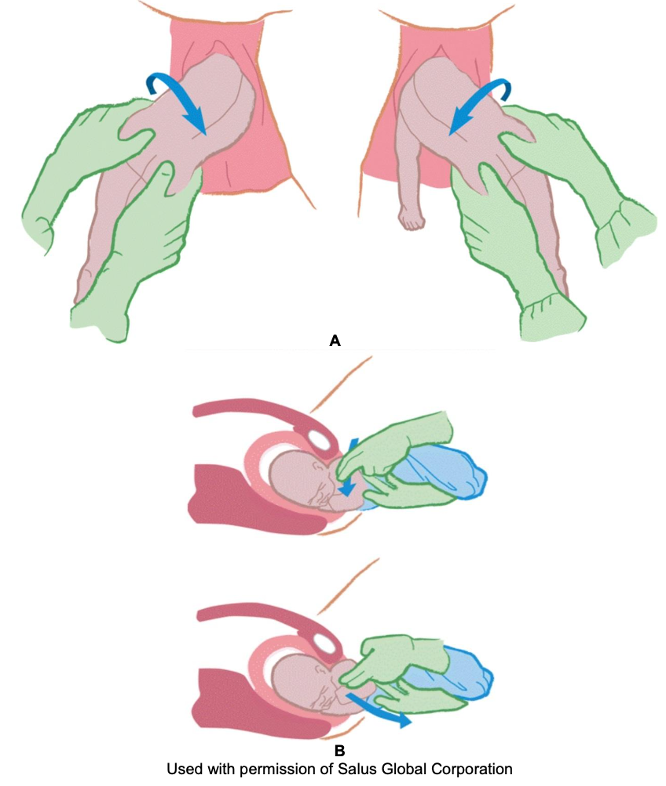
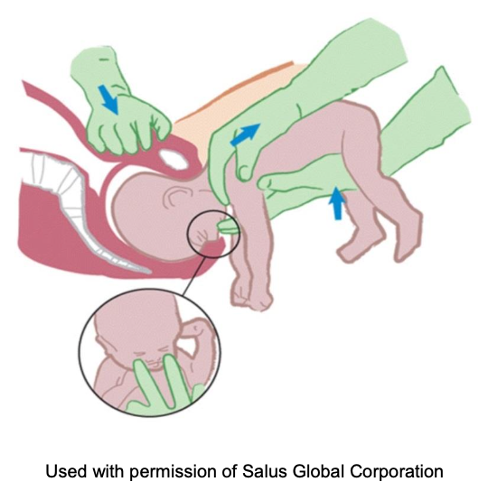
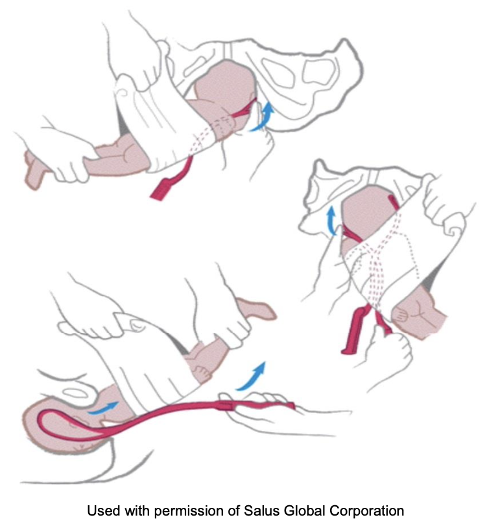
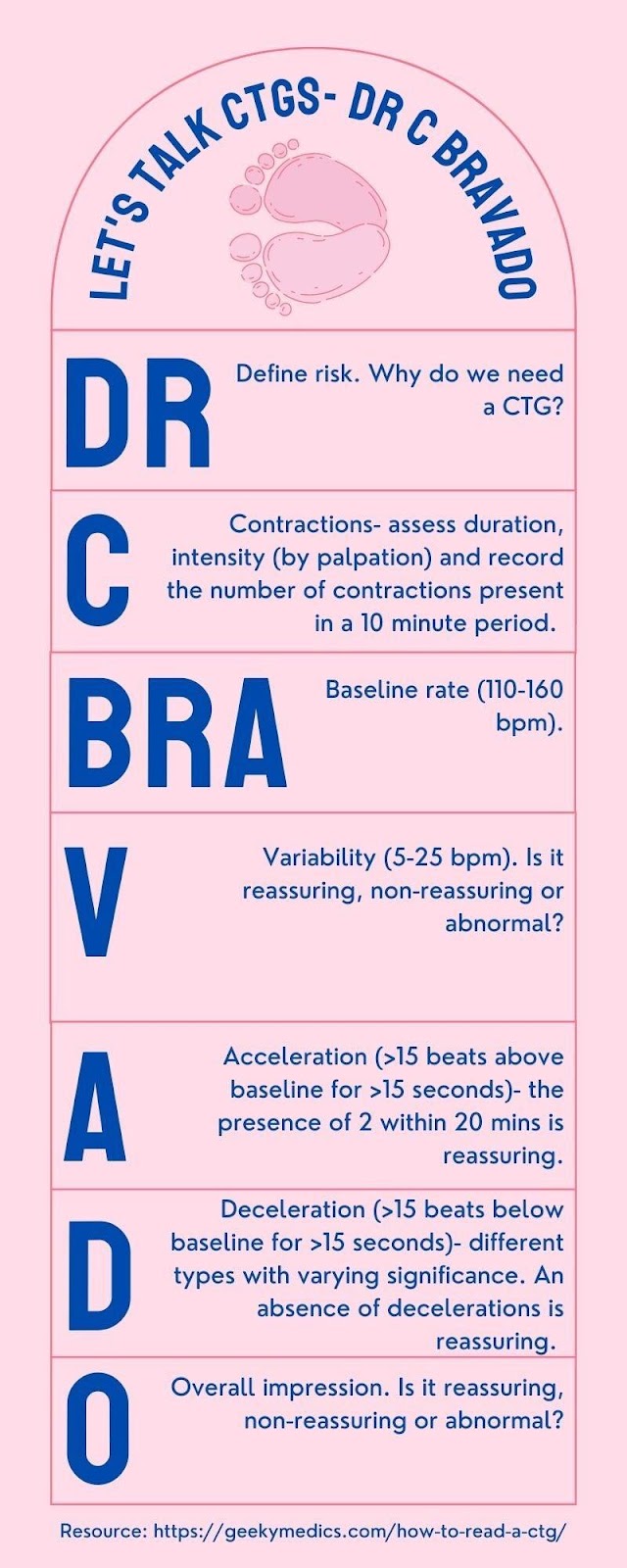

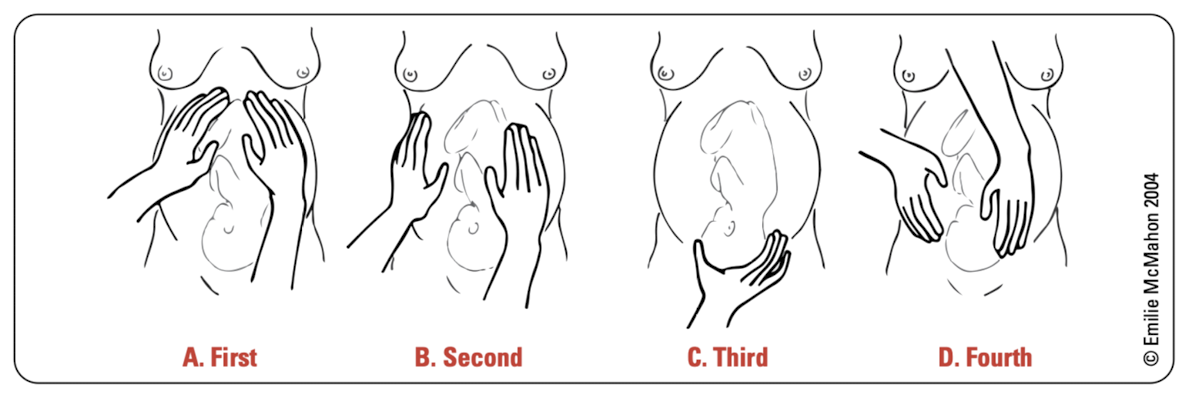
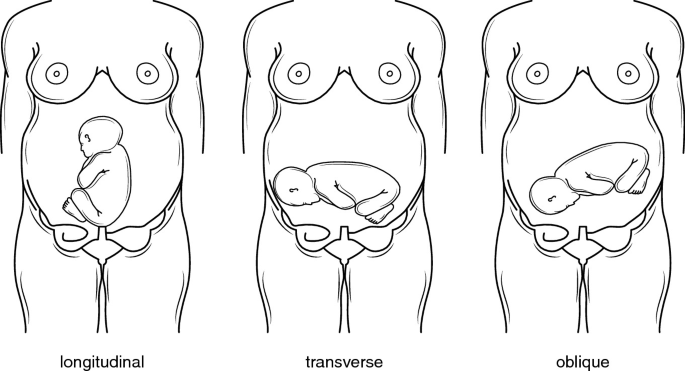
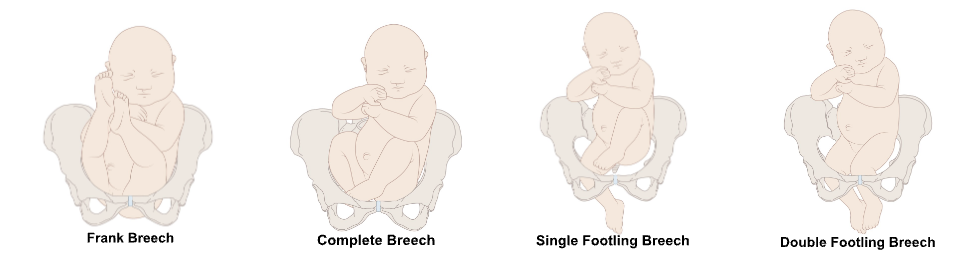
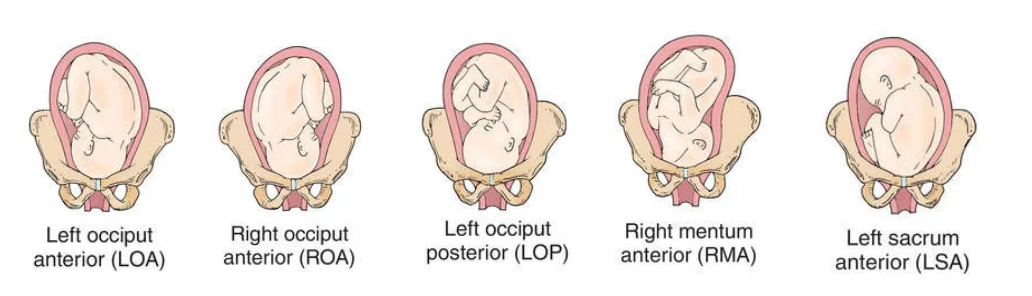
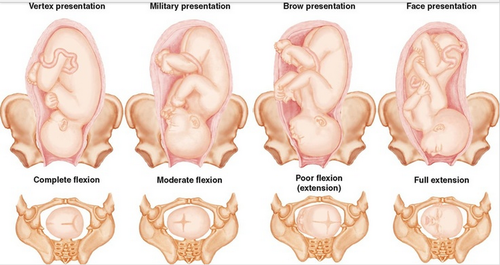
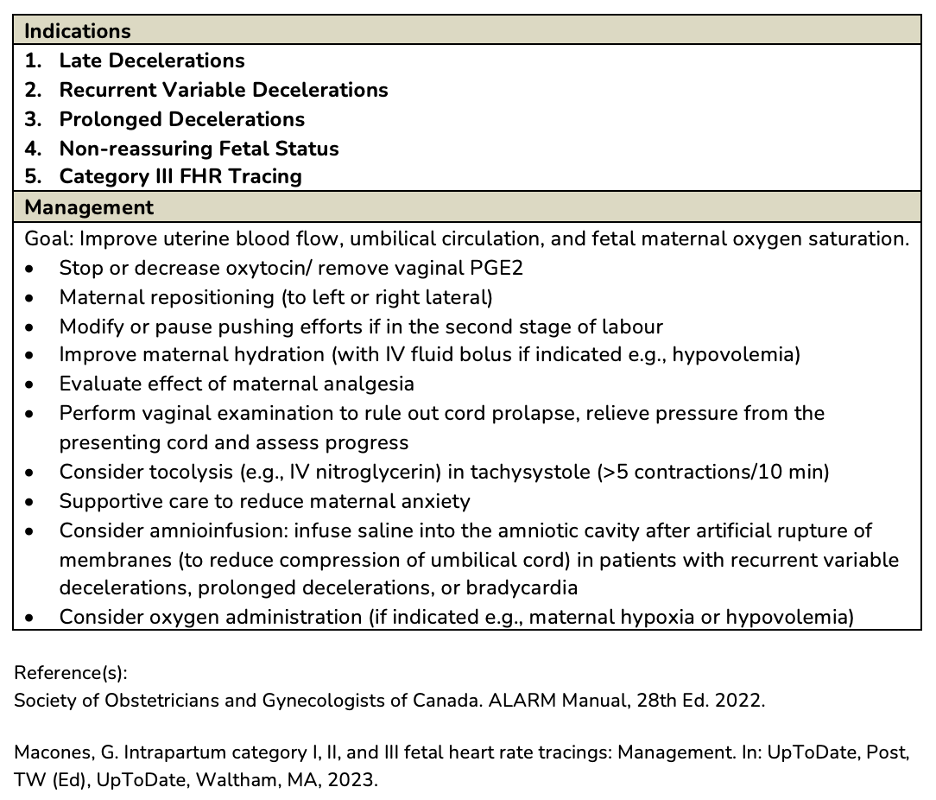
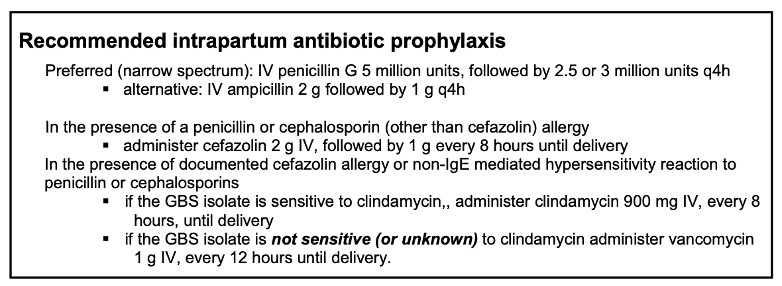


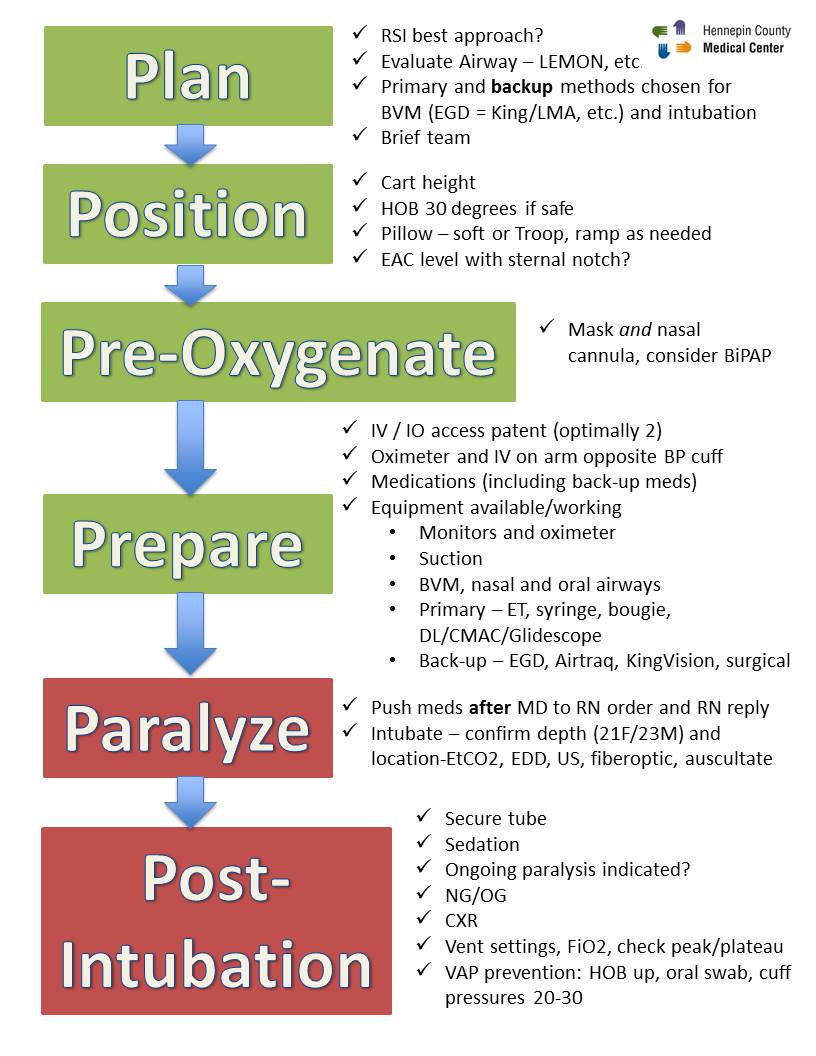{kind=link}