18 m/o presents with a head injury following an unwitnessed fall from height. Will develop signs of increasing ICP progressing to herniation (secondary to epidural hematoma).
An 18-month-old presents to the ED at a community hospital with a head injury following an unwitnessed fall from significant height with initial loss of consciousness. Presents irritable but stable, and subsequently develops signs of increasing ICP progressing to herniation (secondary to an epidural hematoma).
Overall Goal: Practice management of pediatric traumatic brain injury
Specific Learning Objectives:
Time Recommended: 60 minutes total (10 min Setup | 25 min Scenario | 25 min Debrief)
Patient Recommendation: Toddler Manikin if possible
Medical Equipment:
Medications:
| Role | Description (Role, Behaviour, Key Moments, Script) |
| Emerge RN |
Skillful and helpful. Review patient notes from triage, provide support with monitor application, IV start, medication administration, lab results. If not recognized by learner, prompt-
|
Moulage: Boggy swelling to left parietal scalp if possible, some blood on head.
Set-Up: Patient not yet on any monitors. Is alone in on bed in room, as mother went to bring her other children to their grandparents.
Note: While prepping for your simulation, don't forget to prep for the debrief. Become comfortable with your chosen framework, review your objectives. For additional debriefing resources, see our Resources page.
Credits:
Original Authors: Dr. Diana De Santis, Dr. Jennifer Klowak, Dr. Quan
Date: 2020
Originally published on: EM Sim Cases
Most Recent Modification: Mateo Orrantia
Modified by: 2021
A good prebriefing is an essential component of running effective simulations, as it sets the stage for everything that comes after it1-3. An effective prebrief will create a safe container for learning, and in doing so, help participants feel more comfortable pushing their limits, sharing their thoughts and feelings, and buying into the experience. In turn, this will enhance engagement, participation, and learning. To that end, the prebriefing process needs to cover a lot of information1-5, which can make it daunting to novice or non-expert facilitators. To help, we have consulted the relevant literature and put together a prebrief guide to ensure that you have the tools you need to run an effective pre-briefing session.
Throughout the pre-brief, it is important that you convey your commitment to respecting learners and their perspective2-4, and establish and maintain the simulation as a safe space for learning1,4,5.
Prebrief Guide (Sample Phrases in Italics)
Welcome learners. Introduce yourself, your role, and your experience with simulation.
Go over the time requirements for the simulation, when breaks will occur, how learners should handle incoming calls or texts, etc.
Clarify the learning objectives for the simulation1-5. Give information on the purpose of the simulation without giving out specific actions or information that might compromise the learning experience for participants.
Explain how participants will be evaluated (formative/summative/not evaluated). Briefly discuss the debrief process that will take place at the end of the simulation.
Give details on what expectations are for the learners' behaviour during the simulation, setting basic ground rules2-5. Go over expectations for yourself as the facilitator. Reinforce the simulation as a learning environment, where mistakes aren't something to be punished but opportunities for further learning.
This could be a good place to pause and ask learners if they have any additional expectations, fears, comments, or questions about the topic for the day.
Ensure all participants agree to the confidentiality expectations of the simulation. Often, this will follow the mantra of "What happens in the simulation stays in the simulation," where learners and instructors agree not to share information on others' performance or scenario details outside of the simulation environment.
Explain that you've done what you can to make the simulation as real as possible, but acknowledge the limitations. Ask the learner to commit to doing what they can to act as if everything was real, explaining that the quality of their learning will depend on their willingness to participate as fully as possible. For the first simulation with a new group, it could be helpful to explain the importance of a mutual fiction contract.
Explain the different roles in the simulation and assign learners to them. If you have predetermined scripts for certain roles, hand them out here.
Explain the resources that will be available for the participants to use, how they should call for help in the simulation, what your role will be in providing information.
Orient participants to simulation space, equipment, manikin, etc. This can also be done by allowing participants to explore the simulation space and manikin for themselves.
Ask for questions!
References
1. Rudolph JW, Raemer DB, Simon R. Establishing a safe container for learning in simulation: the role of the presimulation briefing. Simul Healthc. 2014 Dec;9(6):339-49. doi: 10.1097/SIH.0000000000000047. PMID: 25188485.
2. Leigh G, Steuben F. Setting Learners up for Success: Presimulation and Prebriefing Strategies. Teaching and Learning in Nursing. 2018; 13(3):185-189. https://doi.org/10.1016/j.teln.2018.03.004
3. Lecomte F, Jaffrelot M. Chapter 33 - Prebriefing and Briefing. Clinical Simulation. 2019; 2nd ed.; 471-482. https://doi.org/10.1016/B978-0-12-815657-5.00034-6.
4. INACSL Standards Committee (2016, December). INACSL standards of best practice: SimulationSM Facilitation. Clinical Simulation in Nursing, 12(S), S16-S20. http://dx.doi.org/10.1016/j.ecns.2016.09.007.
5. Simon R, Raemer D, Rudolph J. Rater's handbook for the Debriefing Assessment for Simulation in Healthcare (DASH) Rater Version. 2009. http://www.harvardmedsim.org/debriefing-assesment-simulation-healthcare.php.
An 18-month old boy is brought to Emerge by his mother after falling off of backyard playground equipment. After bringing him, the mom left to bring her other children to their grandparents, who live on the outside of town.
|
Patient Chart |
|||||||||
|
Patient Name: Sam |
Age: 18mo |
Gender: M |
Weight: 12.5kg |
||||||
|
Presenting complaint: Head injury |
|||||||||
|
Temp: 37oC |
HR: 145 |
BP: 90/50 |
RR: 35 |
O2Sat: 98% |
FiO2: room air |
||||
|
Cap glucose: 4 |
GCS: 11 (E3 V3 M5) |
||||||||
|
Triage Note: Brought to ER by mom after fall off playground (approx. 6ft). Mom heard bang and |
|||||||||
|
Allergies: None |
|||||||||
|
Past Medical History: None |
Current Medications: None |
||||||||
Further History: Getting further history impossible.
| Physical Exam | |
| Cardio: Tachycardic, capillary refill 2 seconds | Neuro: Pupils 4mm and reactive. Quiet, moaning, cries with painful stimuli |
| Resp.: Clear breath sounds bilaterally | Head & Neck: Boggy Hematoma left parietal scalp |
| Abdo: Normal | MSK/Skin: Bruise on Abdomen |
| Other: Nil | |
An 18-month old boy is brought to Emerge by his mother after falling off of backyard playground equipment. After bringing him, the mom left to bring her other to their grandparents, who live on the outside of town.
|
Patient Chart |
|||||||||
|
Patient Name: Sam |
Age: 18mo |
Gender: M |
Weight: 12.5kg |
||||||
|
Presenting complaint: Head injury |
|||||||||
|
Temp: 37oC |
HR: 145 |
BP: 90/50 |
RR: 35 |
O2Sat: 98% |
FiO2: room air |
||||
|
Cap glucose: 4 |
GCS: 11 (E3 V3 M5) |
||||||||
|
Triage Note: Brought to ER by mom after fall off playground (approx. 6ft). Mom heard bang and |
|||||||||
|
Allergies: None |
|||||||||
|
Past Medical History: None |
Current Medications: None |
||||||||
Patient is quiet and moaning. Cries with painful stimulus.
| Patient State/Vitals | ||||||
| Rhythm: Sinus tach | HR: 145 | BP: 90/50 | RR: 35 | |||
| O2SAT: 98% | T: 37oC | GCS: 11 | AVPU: Verbal | |||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Place monitors |
Time Passes ⇒ Gradual Progression |
4 Minutes or all actions complete ⇒ 2. Increased ICP |
Further History: Getting further history impossible.
| Physical Exam | |
| Cardio: Tachycardic, capillary refill 2 seconds | Neuro: Pupils 4mm and reactive. Quiet, moaning, cries with painful stimuli |
| Resp.: Clear breath sounds bilaterally | Head & Neck: Boggy Hematoma left parietal scalp |
| Abdo: Normal | MSK/Skin: Bruise on Abdomen |
| Other: Nil | |
The lab results are fairly unremarkable, and do not show anything that should be of particular concern to this scenario.
| Sam | |||||
| MRN: 1234-567-890 | Age: 18mo | ||||
| Complete Blood Count | |||||
| WBC | 8 | x109L | |||
| Hgb | 130 | g/L | L | ||
| Plt | 200 | x109L | |||
| Electrolytes | |||||
| Na | 140 | mmol/L | |||
| K | 4.4 | mmol/L | |||
| Cl | 100 | mmol/L | |||
| Urea | 5 | mmol/L | |||
| Cr | 30 | µmol/L | L | ||
| Glucose | 4 | mmol/L | |||
| Extended Electrolytes | |||||
| Ca | 2.2 | mg/dL | L | ||
| Mg | 0.9 | mEq/L | L | ||
| PO4 | 1.5 | mmHg | L | ||
| Venous Blood Gas | |||||
| pH | 7.3 | L | |||
| pCO2 | 48 | mmHg | |||
| PO2 | 80 | mmHg | H | ||
| HCO3 | 22 | meQ/L | |||
| Lactate | 1 | mmol/L | |||
| Cardiac/Coagulants | |||||
| INR | 1 | ||||
| aPTT | 30 | s | L | ||
| Biliary | |||||
| AST | 20 | IU/L | |||
| ALT | 20 | IU/L | |||
| GGT | 15 | IU/L | |||
| Bili | 2 | µmol/L | |||
| Lipase | 10 | IU/L | |||
| Tox | |||||
| EtOH | Neg | ||||
| ASA | Neg | ||||
| Tylenol | Neg | ||||
| Patient State/Vitals | ||||||
| Rhythm: Sinus brady | HR: 55 (↓) | BP: 140/100 (↑) | RR: 12 (irregular) (↓) | |||
| O2SAT: 93% (↓) | T: 37oC | GCS: 5 (E1 V1 M3) (↓) | AVPU: Pain | |||
| Sam | |||||
| MRN: 1234-567-890 | Age: 18mo | ||||
| Complete Blood Count | |||||
| WBC | 8 | x109L | |||
| Hgb | 130 | g/L | L | ||
| Plt | 200 | x109L | |||
| Electrolytes | |||||
| Na | 140 | mmol/L | |||
| K | 4.4 | mmol/L | |||
| Cl | 100 | mmol/L | |||
| Urea | 5 | mmol/L | |||
| Cr | 30 | µmol/L | L | ||
| Glucose | 4 | mmol/L | |||
| Extended Electrolytes | |||||
| Ca | 2.2 | mg/dL | L | ||
| Mg | 0.9 | mEq/L | L | ||
| PO4 | 1.5 | mmHg | L | ||
| Venous Blood Gas | |||||
| pH | 7.3 | L | |||
| pCO2 | 48 | mmHg | |||
| PO2 | 80 | mmHg | H | ||
| HCO3 | 22 | meQ/L | |||
| Lactate | 1 | mmol/L | |||
| Cardiac/Coagulants | |||||
| INR | 1 | ||||
| aPTT | 30 | s | L | ||
| Biliary | |||||
| AST | 20 | IU/L | |||
| ALT | 20 | IU/L | |||
| GGT | 15 | IU/L | |||
| Bili | 2 | µmol/L | |||
| Lipase | 10 | IU/L | |||
| Tox | |||||
| EtOH | Neg | ||||
| ASA | Neg | ||||
| Tylenol | Neg | ||||
Patient stops crying and GCS declines, develops signs of Cushing's triad (HTN, Bradycardia, Irregular respirations). Right pupil is 4mm and sluggish, left pupil is 8mm and unreactive.
| Patient State/Vitals | ||||||
| Rhythm: Sinus brady | HR: 55 (↓) | BP: 140/100 (↑) | RR: 12 (irregular) (↓) | |||
| O2SAT: 93% (↓) | T: 37oC | GCS: 5 (E1 V1 M3) (↓) | AVPU: Pain | |||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Re-examine patient given clinical change |
No BVM ⇒ O2SAT 80% |
Decision to Intubate⇒ 3. Intubation |
| Patient State/Vitals | ||||||
| Rhythm: Sinus brady | HR: 55 (↓) | BP: 140/100 (↑) | RR: 12 (irregular) (↓) | |||
| O2SAT: 93% (↓) | T: 37oC | GCS: 5 (E1 V1 M3) (↓) | AVPU: Pain | |||
Cushing's Triad: Cushing's Triad is a set of three primary signs that often indicate an increased ICP. They are: a change in respirations - often irregular and deep, a widening pulse pressure, and bradycardia.
Clinical Findings Indicating Elevated ICP in Children:
Reference
1. Robert C Tasker. Elevated Intracranial Pressure (ICP) in Children: Clinical Manifestations and Diagnosis. UpToDate. 13 Feb 2020. Elevated intracranial pressure (ICP) in children: Clinical manifestations and diagnosis - UpToDate
EARLY INVOLVEMENT OF A NEUROSURGEON SHOULD OCCUR FOR ALL CHILDREN WITH SIGNS OF INCREASED ICP OR HERNIATION, IF POSSIBLE
| General Measures for Stabilization and Management of Increased ICP |
|
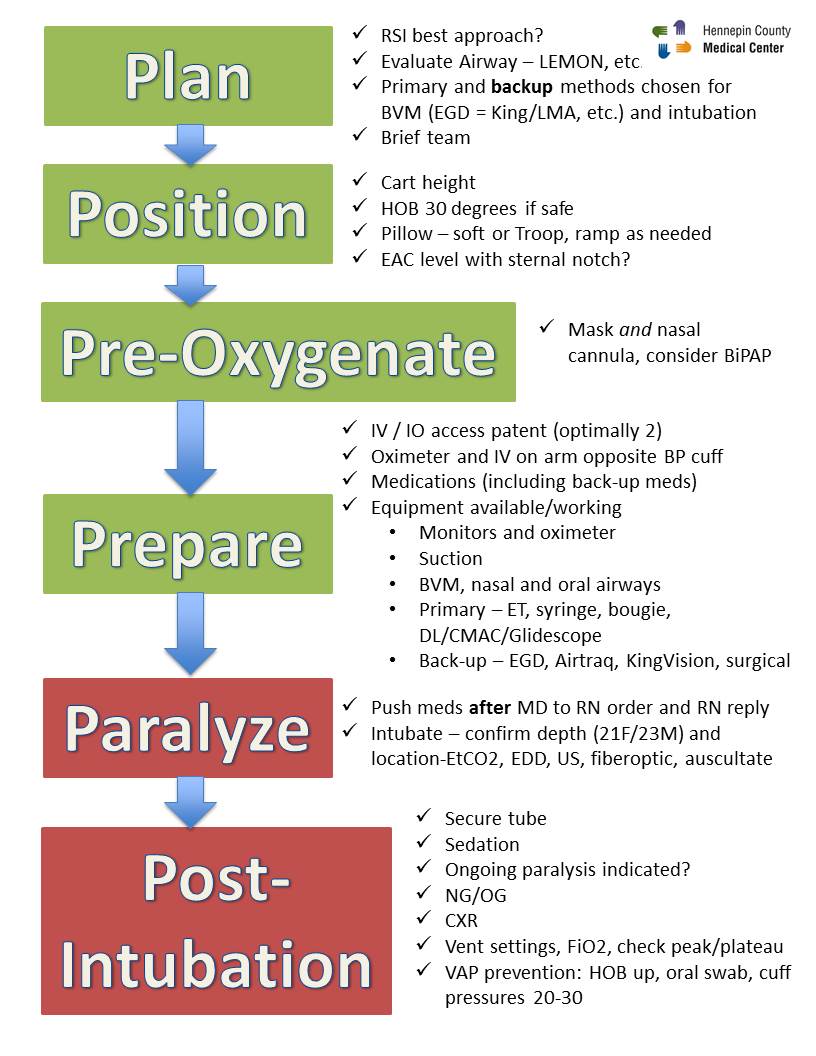
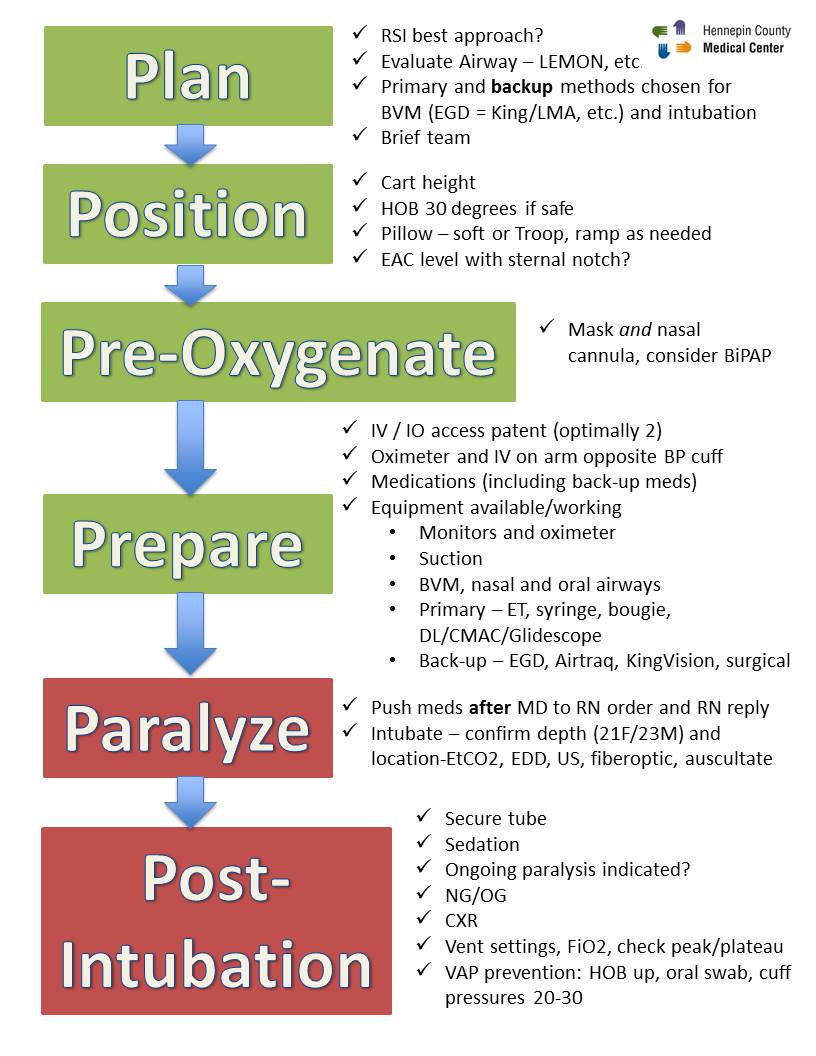
1. Secure the airway with RSI (using C-Spine immobilization in trauma patients) for the following:
Maintain PaCO2 at 35 to 40mmHg in intubated patients, unless signs of herniation |
| 2. Rapid treatment of hypoxia, hypercarbia, hypotension, maintain normal oxygenation |
| 3. Check for, and treat, hypoglycemia + Maintain hemoglobin >70g/L |
| 4. Elevate head 15-30 degrees and keep head midline |
| 5. Aggressively treat fever using antipyretics or cooling blankets |
| 6. Maintain paralysis and control shivering using muscle relaxants (vecuronium, rocuronium) |
| 7. Administer prophylactic anticonvulsants (levetiracetam, phenytoin, phenobarbital) to those who are at high risk of seizure (severe TBI, depressed skull fracture, parenchymal abnormalities) |
| 8. Maintain adequate analgesia (to blunt response to noxious stimuli) and sedation |
|
9. For Intubated Patients:
|
References
1. Robert Tasker. Elevated Intracranial Pressure (ICP) in Children: Management. UpToDate. 4 January 2021. Elevated intracranial pressure (ICP) in children: Management - UpToDate
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 60 (↑) | BP: 130/90 (↓) | RR: 12 | |||
| O2SAT: 93% | T: 37oC | GCS: 5 (E1 V1 M3) | ||||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Verbalize airway plan including airway |
Mannitol or hypertonic saline ⇒ Left |
Intubation complete ⇒ 4. Disposition |
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 60 (↑) | BP: 130/90 (↓) | RR: 12 | |||
| O2SAT: 93% | T: 37oC | GCS: 5 (E1 V1 M3) | ||||
Patient paralyzed, and there is an improvement in vital signs. Pupils are now 4mm and reactive.
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 100 (↑) | BP: 110/90 (↓) | RR: per vent | |||
| O2SAT: 98% (↑) | T: 37oC | GCS: 2T (↓) | AVPU: Unresponsive | |||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Choose appropriate sedation |
No Modifiers for this Stage | Transfer arranged ⇒ Debrief |
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 100 (↑) | BP: 110/90 (↓) | RR: per vent | |||
| O2SAT: 98% (↑) | T: 37oC | GCS: 2T (↓) | AVPU: Unresponsive | |||
Choosing a Debrief Framework:
A good debrief has been identified in the literature as the most important part of a successful simulation experience. If you're a novice or inexperienced facilitator, use this table to help you choose which debrief framework you want to use, just tap the button on their name and you will be directed to the appropriate aids or scripts. While we recommend the PEARLS framework, take a look to see if there may be another that is a better fit for your situation.
|
|
|||||
|
Time |
Facilitator Level |
Prep Time |
Scenario Type |
Flexibility |
|
|
Moderate |
Novice |
Moderate |
Any |
High |
|
|
Short-Moderate |
Novice |
Low |
Short w/ Clear Objectives |
Low |
|
|
Moderate |
Novice |
Moderate |
Any, esp. Team-focused |
Moderate |
|
|
Very Short |
No experience |
None |
Any |
Low |
|
|
Short |
Novice |
Low |
Low number of non-technical skills |
Low |
|
|
Very Short |
No experience |
None |
Any |
Moderate |
|
|
Moderate-Long |
Novice |
Moderate |
Any |
Moderate |
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Objective |
Task |
Sample Phrases |
||
|
1. Setting the Scene |
Create a safe context for learning |
State the goal of debriefing; articulate the basic assumption |
“Let’s spend X minutes debriefing. Our goal is to improve how we work together and care for our patients.” “Everyone here is intelligent and wants to improve”
|
||
|
2. Reactions |
Explore feelings |
Solicit initial reactions and emotions
|
“Any initial reactions?” “How are you feeling?” |
||
|
3. Description |
Clarify Facts |
Develop a shared understanding of the case |
“Can you please share a short summary of the case?” “What was the working diagnosis? Does everyone agree?”
|
||
|
4. Analysis |
Explore a variety of performance domains:
|
See bottom of guide for details on the analysis phase |
For each item to be debriefed: 1. Preview Statement: (to introduce topic)
2. Pick Analysis method + Analyze: (see below for more info on each method)
3. Mini Summary: (to summarize discussion of topic)
Phase Wrap-up: "Any outstanding issues or concerns before we start to close?" |
||
|
5. Application or Summary |
Identify take-aways |
Can be learner- or instructor-centered |
Learner-centered: “What are some takeaways from this discussion for our clinical practice?”
Instructor-centered: “The key learning points for the case were [insert learning points]”
|
||
|
Analysis Phase Details |
|||||
|
Choose an analysis approach (Different approaches can be used for different topics within the same analysis stage): |
|||||
|
Approach |
Objective |
Sample Phrases |
|||
|
Learner Self-Assessment
|
Promote reflection by asking learners to assess their own performance |
“What aspects were managed well and why?”
“What aspects do you want to change and why?”
|
|||
|
Focused Facilitation
|
Probe deeper on key aspects of performance, uncover mental frames guiding performance |
Use Advocacy-Inquiry Method Advocacy: "I saw [observation], I think [your point-of-view]” "I noticed [observation] I liked that/I was concerned..." Inquiry: “How do you see it? What were your thoughts at the time?” |
|||
|
Provide Information
|
Teach to close clear knowledge gaps as they emerge and provide directive feedback as needed |
“I noticed[behaviour]. Next time you may want to consider [suggested behaviour], because [rationale]” |
|||
PDF from debrief2learn.org: Here
Visual Guide: debrief2learn.org
Alternative Script: Here
Originally Created by: Bajaj K, Meguerdichian M, Thoma B, Huang S, Eppich W, Cheng A. The PEARLS Healthcare Debriefing Tool. Acad Med. 2018, 93(2), 336.
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Goal |
Actions |
Possible Scripts |
|
Gather (Listen)
25% |
|
|
How do you feel? |
|
How do you think it went? Can you tell me what happened? |
||
|
Can anyone add anything to that account? |
||
|
Analyze (Guide Reflection)
50% |
|
|
I noticed… |
|
I noticed…. What was the thought process behind…. When….happened, I saw….What do you think….. I saw…I think….How do you see it? |
||
|
Tell me more about… How did you feel about…. I understand, but tell me about X aspect of the scenario |
||
|
Summarize (Help gather Conclusions)
25%
|
|
|
What are two things that you thought were effective or went well? |
|
What do you think are some areas you/your team need to work on? |
||
|
In today’s session, we…. Going forward, we should…. |
References/Adapted From:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
Instructions:
|
Actions |
Gather |
Analyze |
Summarize |
|
Closed-loop communication
Clear Messages
Clear Roles
Knowing one’s limitations
Knowledge Sharing
Constructive Intervention
Reevaluation and Summarizing
Mutual Respect
|
Student Observations
Instructor Observations
|
Done Well
Needs Improvement
|
Student-led Summary
Instructor-led Summary
|
References/Adapted from:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
|
Set learning objectives |
|
After Case |
How did it go? Address Concerns Review learning points Plan ahead |
Framework from:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Diamond Debrief: Sample Phrases |
|
Description |
|
“So what happened?...and then what happened next?”
Continue asking until confident that the details of the scenario have been raised by the learners
“Let’s not judge our performance now, let’s just focus on what happened” |
|
Transition |
|
“This scenario was designed to show…”
“Let’s address technical and clinical questions. What is the protocol for…?”
“How do we normally deal with this clinical situation?”
“Everyone ok with that?” |
|
Analysis |
|
“How did that make you feel?” To participants, then group “Why?” Then use silence
“How did you/they do that exactly?” “Why did you respond in that way? “ or “Why did you take that action?”
“It feels like…was an issue. Did it feel like that to you?” What I’m hearing from you is…is that correct?”
“This is part of…” (identify the non-technical skill/human factor) “We refer to that as a human factor or non-technical skill, which means…” |
|
Transition |
|
“So, what we’ve talked about in this scenario is…” “What have we agreed we could do?” |
|
Application |
|
“What other kinds of situations might you face that might be similar? How are they similar?”
“How might these skills we discussed play out in those situations?”
“What are you going to do differently in your practice going forward?” |
|
Underlying Principles |
|
Description |
|
Reinforce a safe learning environment. Situate the debrief in the shared and meaningful activity that occurred. Keep the focus dispassionate—discuss what happened but avoid focus on emotions. Listen for emotional responses but resist the temptation to discuss emotions. Make sure everyone shares the same understanding of what happened.
|
|
Transition |
|
Transition into analysis by clarifying any technical and clinical issues |
|
Analysis |
|
Spend most of your time in Analysis. Deconstruct behaviours into specific actions, and explore what happened in detail. Ask about affective responses and validate them. Analyze and interpret the activity by applying appropriate frameworks or lenses (such as non-technical skills, or the clinical context surrounding the scenario). Keep discussion positive, and avoid the temptation to focus on “strengths and weaknesses”. Reflect responses back, allowing participants to amend or augment. |
|
Transition |
|
Transition into Application by reinforcing learning. |
|
Application |
|
Focus on moving from the specifics of the scenario to the more general world of practice. Break behaviours down into specific actions. Explore the other kinds of situations that these might apply to. Ask what participants will do differently in their practice. |
Adapted From: Jaye P, Thomas L, Reedy G (2015). 'The Diamond': a structure for simulation debrief. The Clinical Teacher 12(1). 171-175. onlinelibrary.wiley.com/doi/full/10.1111/tct.12300
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
Pluses:
Deltas:
|
Plus (+) |
Delta (∆) |
References:
((To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Purpose |
Process |
Sample Phrases |
|
Reactions |
|
|
How are you feeling? What are some initial reactions to what just happened? So, in that scenario… |
|
Analysis |
|
1. Observe an event or result. Comment on the observation.
2. Advocate for your position |
I saw that… I think… I noticed that…To me…
I saw…I’m concerned that… |
|
3. Investigate basis for learner’s thinking that led to the observed event or result |
What do you think? Why do you think that happened? How do you see it? What was the thought process behind….? |
||
|
4. Close the gap through discussion and didactics |
I hear…. What would it take for you to do this next time? How could we do this differently next time? I think a few good ideas that came up were… I’d like to say a little bit about…from my experience/literature |
||
|
Summary |
|
|
What are some takeaways from today? What went well today? What would you do differently next time?
In today’s session, we…. Going forward, we should… |
Adapted from:
1. Cushing's Triad is a set of three primary signs that often indicate an increased ICP. They are: a change in respirations - often irregular and deep, a widening pulse pressure, and bradycardia.
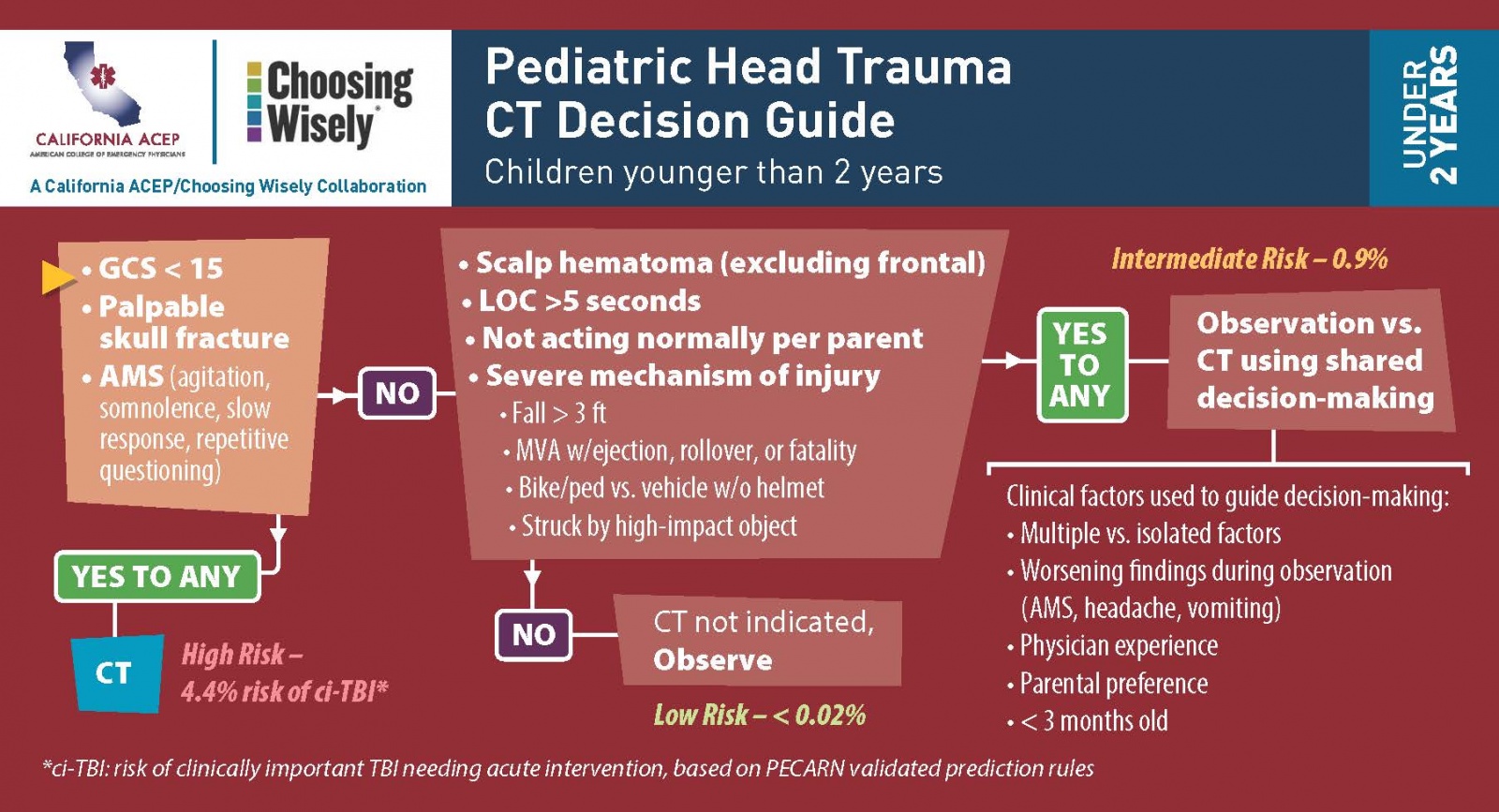
2. When evaluating whether or not a pediatric patient may have a clinically important traumatic brain injury and require a CT, consider the PECARN Head CT Rule (click to open larger in a new window):
 |
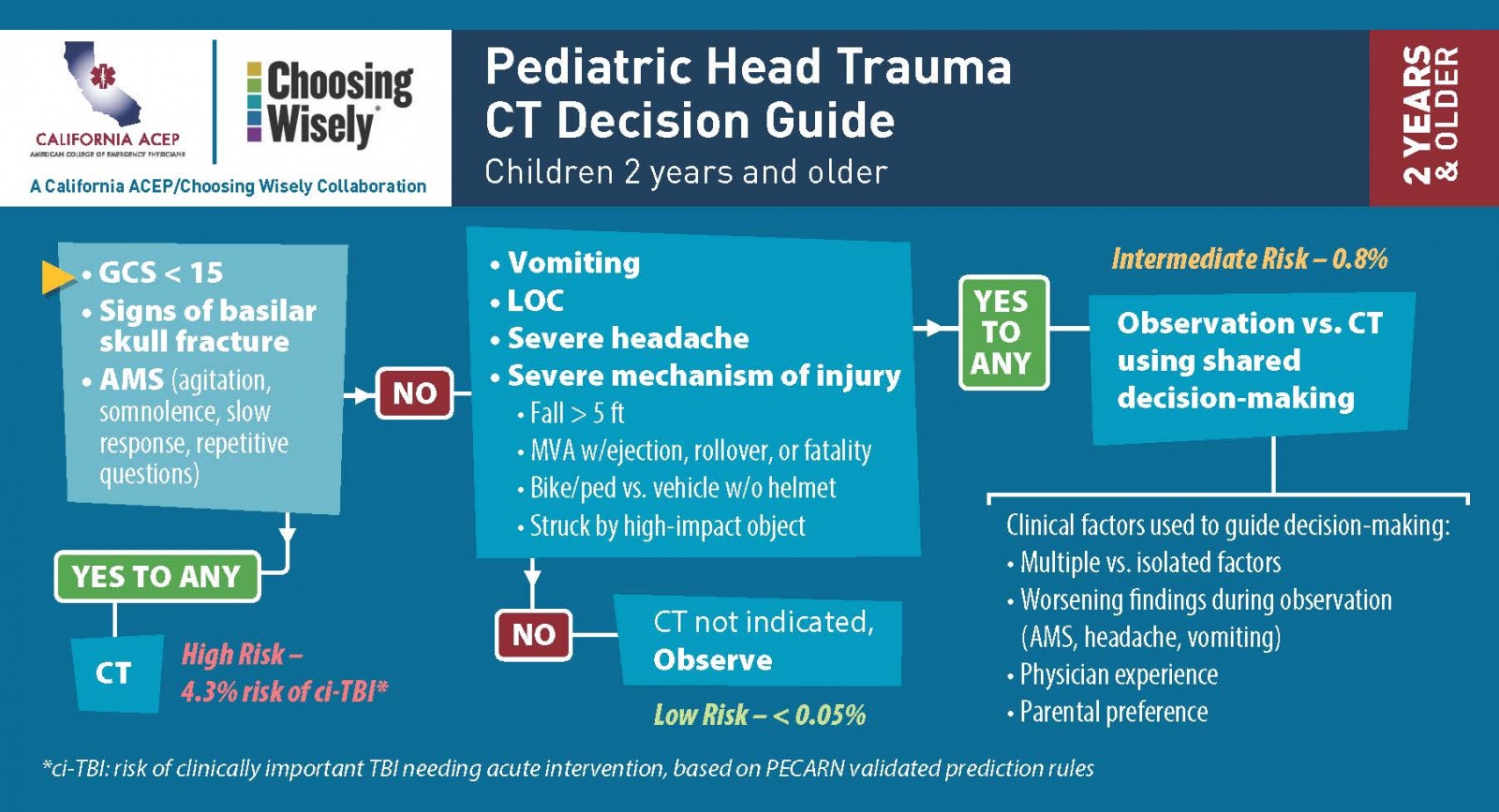 |
Source: PECARN - California ACEP
{kind=link}