Elderly patient arrives via EMS in severe respiratory distress. He becomes increasingly distressed and agitated, requiring intubation. The patient develops a tension pneumothorax and may arrest.
An elderly patient has just arrived via EMS in severe respiratory distress. He has a history of COPD and is on home O2. He's had 3 days of worsening cough, sputum, and dyspnea. He becomes increasingly distressed and agitated, requiring intubation. Learners may consider non-invasive positive pressure ventilation (NIPPV), delayed sequence intubation (DSI), but the patient will ultimately require intubation. Shortly after intubation, the patient becomes very difficult to bag and then becomes hypotensive. If not identified, the patient arrests from a tension pneumothorax.
Overall Goal: Appropriately manage the patient with a severe COPD exacerbation, with consideration of delayed sequence intubation, and recognition/management of the potential complications of positive pressure ventilation (PPV) in this patient subset.
Specific Learning Objectives:
Time Recommended: 40 minutes total (10 min Setup | 15 min Scenario | 15 min Debrief)
Patient Recommendation: Intubatable Mannequin
Medical Equipment:
Medications:
| Role | Description (Role, Behaviour, Key Moments, Script) |
| Bedside RN |
You are a skillful and cooperative bedside RN. Stage 2-
Stage 3/4
|
Moulage: No moulage necessary
Set-Up: The patient should arrive in a similar way to if he had actually been brought by EMS. Do not have any monitors attached at case onset. The facilitator should ensure that all the necessary equipment and medications are accessible in the simulation room.
Note: While prepping for your simulation, don't forget to prep for the debrief. Become comfortable with your chosen framework, review your objectives. For additional debriefing resources, see our Resources page.
Credits:
Original Author: Lindsey McMurray
Date: March 14th 2018
Originally published on: EM SIM cases (Nightmares Course – EM Sim Cases)
Most Recent Modification: June 21st 2021
Modified by: Mateo Orrantia
A good prebriefing is an essential component of running effective simulations, as it sets the stage for everything that comes after it1-3. An effective prebrief will create a safe container for learning, and in doing so, help participants feel more comfortable pushing their limits, sharing their thoughts and feelings, and buying into the experience. In turn, this will enhance engagement, participation, and learning. To that end, the prebriefing process needs to cover a lot of information1-5, which can make it daunting to novice or non-expert facilitators. To help, we have consulted the relevant literature and put together a prebrief guide to ensure that you have the tools you need to run an effective pre-briefing session.
Throughout the pre-brief, it is important that you convey your commitment to respecting learners and their perspective2-4, and establish and maintain the simulation as a safe space for learning1,4,5.
Prebrief Guide (Sample Phrases in Italics)
Welcome learners. Introduce yourself, your role, and your experience with simulation.
Go over the time requirements for the simulation, when breaks will occur, how learners should handle incoming calls or texts, etc.
Clarify the learning objectives for the simulation1-5. Give information on the purpose of the simulation without giving out specific actions or information that might compromise the learning experience for participants.
Explain how participants will be evaluated (formative/summative/not evaluated). Briefly discuss the debrief process that will take place at the end of the simulation.
Give details on what expectations are for the learners' behaviour during the simulation, setting basic ground rules2-5. Go over expectations for yourself as the facilitator. Reinforce the simulation as a learning environment, where mistakes aren't something to be punished but opportunities for further learning.
This could be a good place to pause and ask learners if they have any additional expectations, fears, comments, or questions about the topic for the day.
Ensure all participants agree to the confidentiality expectations of the simulation. Often, this will follow the mantra of "What happens in the simulation stays in the simulation," where learners and instructors agree not to share information on others' performance or scenario details outside of the simulation environment.
Explain that you've done what you can to make the simulation as real as possible, but acknowledge the limitations. Ask the learner to commit to doing what they can to act as if everything was real, explaining that the quality of their learning will depend on their willingness to participate as fully as possible. For the first simulation with a new group, it could be helpful to explain the importance of a mutual fiction contract.
Explain the different roles in the simulation and assign learners to them. If you have predetermined scripts for certain roles, hand them out here.
Explain the resources that will be available for the participants to use, how they should call for help in the simulation, what your role will be in providing information.
Orient participants to simulation space, equipment, manikin, etc. This can also be done by allowing participants to explore the simulation space and manikin for themselves.
Ask for questions!
References
1. Rudolph JW, Raemer DB, Simon R. Establishing a safe container for learning in simulation: the role of the presimulation briefing. Simul Healthc. 2014 Dec;9(6):339-49. doi: 10.1097/SIH.0000000000000047. PMID: 25188485.
2. Leigh G, Steuben F. Setting Learners up for Success: Presimulation and Prebriefing Strategies. Teaching and Learning in Nursing. 2018; 13(3):185-189. https://doi.org/10.1016/j.teln.2018.03.004
3. Lecomte F, Jaffrelot M. Chapter 33 - Prebriefing and Briefing. Clinical Simulation. 2019; 2nd ed.; 471-482. https://doi.org/10.1016/B978-0-12-815657-5.00034-6.
4. INACSL Standards Committee (2016, December). INACSL standards of best practice: SimulationSM Facilitation. Clinical Simulation in Nursing, 12(S), S16-S20. http://dx.doi.org/10.1016/j.ecns.2016.09.007.
5. Simon R, Raemer D, Rudolph J. Rater's handbook for the Debriefing Assessment for Simulation in Healthcare (DASH) Rater Version. 2009. http://www.harvardmedsim.org/debriefing-assesment-simulation-healthcare.php.
EMS has just brought this patient to emerge. He is in severe respiratory distress. You are called to the bedside.
|
Patient Chart |
|||||||||
|
Patient Name: Peter Long |
Age: 68 |
Gender: M |
Weight: 60kg |
||||||
|
Presenting complaint: Shortness of Breath |
|||||||||
|
Temp: 37oC |
HR: 150 |
BP: 160/95 |
RR: 30 |
O2Sat: 80% |
FiO2: 100% NRB |
||||
|
Cap glucose: 5mmol/L |
GCS: 11 (E4 V2 M5) |
||||||||
|
Triage Note: Patient arrived via EMS. Severe respiratory distress. |
|||||||||
|
Allergies: NKDA |
|||||||||
|
Past Medical History: COPD (Home O2, 2L) |
Current Medications: Tiotropium |
||||||||
Further History:
Lives alone. 3 days worsening cough, sputum, dyspnea. No further history.
| Physical Exam | |
| General Status: Distressed, sitting up, respiratory distress | |
| Cardio: Normal heart sounds | Neuro: Eyes open, moaning intermittently |
| Resp.: Diffuse wheeze/gasping | Head & Neck: Normal |
| Abdo: Normal | MSK/Skin: Normal |
| Other: n/a | |
The patient is sitting up, distressed. Gasping for air.
On exam, patient has dyspnea and is gasping. The patient should be wheezing and moaning intermittently. No verbal response to questions.
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 150 | BP: 160/95 | RR: 30 | |||
| O2SAT: 80% (2L NP) | T: 37oC | GCS: 11 | ||||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Don appropriate PPE |
NRB administered ⇒ O2 to 85% |
After 3-5 minutes⇒ 2. Agitation |
Further History:
Lives alone. 3 days worsening cough, sputum, dyspnea. No further history.
| Physical Exam | |
| General Status: Distressed, sitting up, respiratory distress | |
| Cardio: Normal heart sounds | Neuro: Eyes open, moaning intermittently |
| Resp.: Diffuse wheeze/gasping | Head & Neck: Normal |
| Abdo: Normal | MSK/Skin: Normal |
| Other: n/a | |
This X-ray is indicative of COPD. In it, we can observe enlarged lungs and a flattened diaphragm.
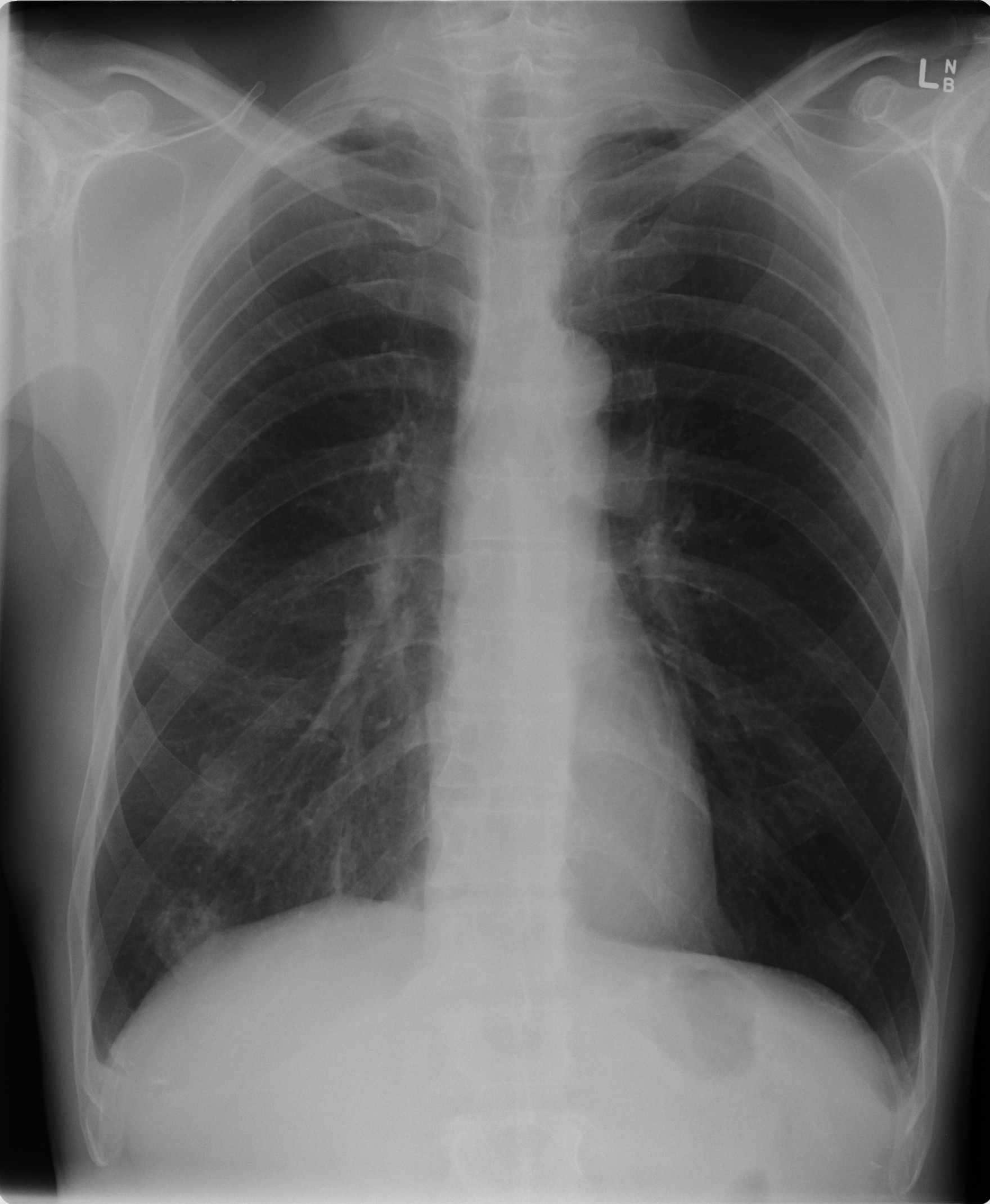
Case courtesy of Townsville radiology training, Radiopaedia.org. From the case rID: 19446
This ECG has many of the features of COPD. Generally, these features include peaked P waves > 2.5 mm in the inferior leads. R waves are absent in SV1-SV2-SV3, and there are low voltages in the left-sided leads (I, aVL, V5-6). Other features are clockwise rotation of the heart with a delayed R/S transition point.

Click to open in new tab (good for showing learners, displaying on screen)
These results are indicative of COPDE, due to very high pCO2 and elevated lactate levels.
| Peter Long | |||||
| MRN: 1234-567-890 | Age: 68 | ||||
| Venous Blood Gas | |||||
| Ref. Range | |||||
| pH | 7.15 | 7.3-7.4 | L | ||
| pCO2 | 80 | mmHg | 40-50 | H | |
| pO2 | 28 | mmHg | 35-40 | ||
| HCO3 | 29 | mEq/L | 22-26 | H | |
| Lactate | 4 | mmol/L | 0.4-2 | H | |
The patient is sitting up, distressed. Gasping for air.
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 120 | BP: 160/95 | RR: 30 | |||
| O2SAT: 80% (neb) | T: 37oC | GCS: 11 | ||||
| Peter Long | |||||
| MRN: 1234-567-890 | Age: 68 | ||||
| Venous Blood Gas | |||||
| Ref. Range | |||||
| pH | 7.15 | 7.3-7.4 | L | ||
| pCO2 | 80 | mmHg | 40-50 | H | |
| pO2 | 28 | mmHg | 35-40 | L | |
| HCO3 | 29 | mEq/L | 22-26 | H | |
| Lactate | 4 | mmol/L | 0.4-2 | H | |
The patient is becoming more agitated and has started grabbing at his face mask
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 130 (↓) | BP: 160/95 | RR: 30 | |||
| O2SAT: 85% (NRB) (↑) | T: 37oC | GCS: 11 | ||||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Consider delayed sequence intubation with |
Ketamine administered ⇒ Patient settles Intubation complete ⇒ O2 to 92%, HR to 90 |
2 min post-intubation ⇒ 3. Pneumothorax |
The patient is becoming more agitated and has started grabbing at their face mask
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 130 (↓) | BP: 160/95 | RR: 30 | |||
| O2SAT: 85% (NRB) (↑) | T: 37oC | GCS: 11 | ||||
Patient develops obstructive shock from pneumothorax
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 130 | BP: 70/50 (↓) | RR: 16 (No air entry R chest) (↓) | |||
| O2SAT: 90% (Vent) (↑) | T: 37oC | GCS: 2T (↓) | ||||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Troubleshoot high airway pressures (D/C from vent, |
Pneumothorax identified and decompressed ⇒ O2 and BP improve |
Pneumothorax identified and decompressed ⇒ Debrief Pneumothorax not identified ⇒ 4. PEA Arrest |
This ultrasound shows pneumothorax. There is a loss of horizontal lung sliding at the parietal pleura. There is also an increased prominence of A-lines (The horizontal lines below the parietal pleura), which also indicates pneumothorax. There is also a loss of the vertical B-lines that would usually be present below the parietal surface.
Source: Lung ultrasound: Pneumothorax • LITFL • Ultraosund Library
| Patient State/Vitals | ||||||
| Rhythm: Sinus | HR: 130 | BP: 70/50 (↓) | RR: 16 (No air entry R chest) (↓) | |||
| O2SAT: 90% (Vent) (↑) | T: 37oC | GCS: 2T (↓) | ||||
This ultrasound shows a normal lung with sliding.
Patient deteriorates, entering PEA arrest.
| Patient State/Vitals | ||||||
| Rhythm: Pulseless Sinus | HR: 140 (↑) | BP: N/A (↓) | RR: 0 (↓) | |||
| O2SAT: 0 (↓) | T: 37oC | GCS: 2T | ||||
| Expected Learner Actions | Modifiers | Triggers |
|---|---|---|
|
Recognize PEA |
Needle Decompression ⇒ Patient Stabilizes |
Organizing transfer ⇒ Debrief |

| Patient State/Vitals | ||||||
| Rhythm: Pulseless Sinus | HR: 140 (↑) | BP: N/A (↓) | RR: 0 (↓) | |||
| O2SAT: 0 (↓) | T: 37oC | GCS: 2T | ||||
|
Potential Cause |
How to Identify |
Treatments |
|
Hypovolemia |
Rapid heart rate and narrow QRS on ECG; other symptoms of low volume |
Infusion of normal saline or Ringer’s lactate |
|
Hypoxia |
Slow heart rate |
Airway management and effective oxygenation |
|
Hydrogen ion excess (acidosis) |
Low amplitude QRS on the ECG |
Hyperventilation; consider sodium bicarbonate bolus |
|
Hypoglycemia* |
Bedside glucose testing |
IV bolus of dextrose |
|
Hypokalemia |
Flat T waves and appearance of a U wave on the ECG |
IV Magnesium infusion |
|
Hyperkalemia |
Peaked T waves and wide QRS complex on the ECG |
Consider calcium chloride, sodium bicarbonate, and an insulin and glucose protocol |
|
Hypothermia |
Typically preceded by exposure to a cold environment |
Gradual rewarming |
|
Tension pneumothorax |
Slow heart rate and narrow QRS complexes on the ECG; difficulty breathing |
Thoracostomy or needle decompression |
|
Tamponade – Cardiac |
Rapid heart rate and narrow QRS complexes on the ECG |
Pericardiocentesis |
|
Toxins |
Typically will be seen as a prolonged QT interval on the ECG; may see neurological symptoms |
Based on the specific toxin |
|
Thrombosis (pulmonary embolus) |
Rapid heart rate with narrow QRS complexes on the ECG |
Surgical embolectomy or administration of fibrinolytics |
|
Thrombosis (myocardial infarction) |
ECG will be abnormal based on the location of the infarction |
Dependent on extent and age of MI |
*Hypoglycemia is not officially one of the H’s and T’s for adults, but it still can be an important cause of PEA, especially in children. If another reversible cause has not been discovered or if the patient is known to be susceptible to hypoglycemia (e.g., brittle diabetes, past surreptitious use of insulin) then this potential cause of PEA should be considered.
Choosing a Debrief Framework:
A good debrief has been identified in the literature as the most important part of a successful simulation experience. If you're a novice or inexperienced facilitator, use this table to help you choose which debrief framework you want to use, just tap the button on their name and you will be directed to the appropriate aids or scripts. While we recommend the PEARLS framework, take a look to see if there may be another that is a better fit for your situation.
|
|
|||||
|
Time |
Facilitator Level |
Prep Time |
Scenario Type |
Flexibility |
|
|
Moderate |
Novice |
Moderate |
Any |
High |
|
|
Short-Moderate |
Novice |
Low |
Short w/ Clear Objectives |
Low |
|
|
Moderate |
Novice |
Moderate |
Any, esp. Team-focused |
Moderate |
|
|
Very Short |
No experience |
None |
Any |
Low |
|
|
Short |
Novice |
Low |
Low number of non-technical skills |
Low |
|
|
Very Short |
No experience |
None |
Any |
Moderate |
|
|
Moderate-Long |
Novice |
Moderate |
Any |
Moderate |
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Objective |
Task |
Sample Phrases |
||
|
1. Setting the Scene |
Create a safe context for learning |
State the goal of debriefing; articulate the basic assumption |
“Let’s spend X minutes debriefing. Our goal is to improve how we work together and care for our patients.” “Everyone here is intelligent and wants to improve”
|
||
|
2. Reactions |
Explore feelings |
Solicit initial reactions and emotions
|
“Any initial reactions?” “How are you feeling?” |
||
|
3. Description |
Clarify Facts |
Develop a shared understanding of the case |
“Can you please share a short summary of the case?” “What was the working diagnosis? Does everyone agree?”
|
||
|
4. Analysis |
Explore a variety of performance domains:
|
See bottom of guide for details on the analysis phase |
For each item to be debriefed: 1. Preview Statement: (to introduce topic)
2. Pick Analysis method + Analyze: (see below for more info on each method)
3. Mini Summary: (to summarize discussion of topic)
Phase Wrap-up: "Any outstanding issues or concerns before we start to close?" |
||
|
5. Application or Summary |
Identify take-aways |
Can be learner- or instructor-centered |
Learner-centered: “What are some takeaways from this discussion for our clinical practice?”
Instructor-centered: “The key learning points for the case were [insert learning points]”
|
||
|
Analysis Phase Details |
|||||
|
Choose an analysis approach (Different approaches can be used for different topics within the same analysis stage): |
|||||
|
Approach |
Objective |
Sample Phrases |
|||
|
Learner Self-Assessment
|
Promote reflection by asking learners to assess their own performance |
“What aspects were managed well and why?”
“What aspects do you want to change and why?”
|
|||
|
Focused Facilitation
|
Probe deeper on key aspects of performance, uncover mental frames guiding performance |
Use Advocacy-Inquiry Method Advocacy: "I saw [observation], I think [your point-of-view]” "I noticed [observation] I liked that/I was concerned..." Inquiry: “How do you see it? What were your thoughts at the time?” |
|||
|
Provide Information
|
Teach to close clear knowledge gaps as they emerge and provide directive feedback as needed |
“I noticed[behaviour]. Next time you may want to consider [suggested behaviour], because [rationale]” |
|||
PDF from debrief2learn.org: Here
Visual Guide: debrief2learn.org
Alternative Script: Here
Originally Created by: Bajaj K, Meguerdichian M, Thoma B, Huang S, Eppich W, Cheng A. The PEARLS Healthcare Debriefing Tool. Acad Med. 2018, 93(2), 336.
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Goal |
Actions |
Possible Scripts |
|
Gather (Listen)
25% |
|
|
How do you feel? |
|
How do you think it went? Can you tell me what happened? |
||
|
Can anyone add anything to that account? |
||
|
Analyze (Guide Reflection)
50% |
|
|
I noticed… |
|
I noticed…. What was the thought process behind…. When….happened, I saw….What do you think….. I saw…I think….How do you see it? |
||
|
Tell me more about… How did you feel about…. I understand, but tell me about X aspect of the scenario |
||
|
Summarize (Help gather Conclusions)
25%
|
|
|
What are two things that you thought were effective or went well? |
|
What do you think are some areas you/your team need to work on? |
||
|
In today’s session, we…. Going forward, we should…. |
References/Adapted From:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
Instructions:
|
Actions |
Gather |
Analyze |
Summarize |
|
Closed-loop communication
Clear Messages
Clear Roles
Knowing one’s limitations
Knowledge Sharing
Constructive Intervention
Reevaluation and Summarizing
Mutual Respect
|
Student Observations
Instructor Observations
|
Done Well
Needs Improvement
|
Student-led Summary
Instructor-led Summary
|
References/Adapted from:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
|
Set learning objectives |
|
After Case |
How did it go? Address Concerns Review learning points Plan ahead |
Framework from:
(To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Diamond Debrief: Sample Phrases |
|
Description |
|
“So what happened?...and then what happened next?”
Continue asking until confident that the details of the scenario have been raised by the learners
“Let’s not judge our performance now, let’s just focus on what happened” |
|
Transition |
|
“This scenario was designed to show…”
“Let’s address technical and clinical questions. What is the protocol for…?”
“How do we normally deal with this clinical situation?”
“Everyone ok with that?” |
|
Analysis |
|
“How did that make you feel?” To participants, then group “Why?” Then use silence
“How did you/they do that exactly?” “Why did you respond in that way? “ or “Why did you take that action?”
“It feels like…was an issue. Did it feel like that to you?” What I’m hearing from you is…is that correct?”
“This is part of…” (identify the non-technical skill/human factor) “We refer to that as a human factor or non-technical skill, which means…” |
|
Transition |
|
“So, what we’ve talked about in this scenario is…” “What have we agreed we could do?” |
|
Application |
|
“What other kinds of situations might you face that might be similar? How are they similar?”
“How might these skills we discussed play out in those situations?”
“What are you going to do differently in your practice going forward?” |
|
Underlying Principles |
|
Description |
|
Reinforce a safe learning environment. Situate the debrief in the shared and meaningful activity that occurred. Keep the focus dispassionate—discuss what happened but avoid focus on emotions. Listen for emotional responses but resist the temptation to discuss emotions. Make sure everyone shares the same understanding of what happened.
|
|
Transition |
|
Transition into analysis by clarifying any technical and clinical issues |
|
Analysis |
|
Spend most of your time in Analysis. Deconstruct behaviours into specific actions, and explore what happened in detail. Ask about affective responses and validate them. Analyze and interpret the activity by applying appropriate frameworks or lenses (such as non-technical skills, or the clinical context surrounding the scenario). Keep discussion positive, and avoid the temptation to focus on “strengths and weaknesses”. Reflect responses back, allowing participants to amend or augment. |
|
Transition |
|
Transition into Application by reinforcing learning. |
|
Application |
|
Focus on moving from the specifics of the scenario to the more general world of practice. Break behaviours down into specific actions. Explore the other kinds of situations that these might apply to. Ask what participants will do differently in their practice. |
Adapted From: Jaye P, Thomas L, Reedy G (2015). 'The Diamond': a structure for simulation debrief. The Clinical Teacher 12(1). 171-175. onlinelibrary.wiley.com/doi/full/10.1111/tct.12300
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
Pluses:
Deltas:
|
Plus (+) |
Delta (∆) |
References:
((To learn more about this debriefing framework, visit our page on Debriefing resources)
If you need help with debriefing Crisis Resource Management skills, check out this infographic from Isaak & Stiegler: View Infographic
|
Phase |
Purpose |
Process |
Sample Phrases |
|
Reactions |
|
|
How are you feeling? What are some initial reactions to what just happened? So, in that scenario… |
|
Analysis |
|
1. Observe an event or result. Comment on the observation.
2. Advocate for your position |
I saw that… I think… I noticed that…To me…
I saw…I’m concerned that… |
|
3. Investigate basis for learner’s thinking that led to the observed event or result |
What do you think? Why do you think that happened? How do you see it? What was the thought process behind….? |
||
|
4. Close the gap through discussion and didactics |
I hear…. What would it take for you to do this next time? How could we do this differently next time? I think a few good ideas that came up were… I’d like to say a little bit about…from my experience/literature |
||
|
Summary |
|
|
What are some takeaways from today? What went well today? What would you do differently next time?
In today’s session, we…. Going forward, we should… |
Adapted from:
1. When troubleshooting high ventilator pressures, think of the DOPE mnemonic:
2. The indications for delayed sequence intubation are:
3. The H's and T's of PEA are
References
1. Scott Weingart, MD FCCM. EMCrit Podcast 16 – Coding Asthmatic, DOPES and Finger Thoracostomy. EMCrit Blog. Published on December 23, 2009. Available at [https://emcrit.org/emcrit/finger-thoracostomy/ ].
2. Chris Nickson. Delayed Sequence Intubation (DSI). Life in The Fast Lane. Published November 3, 2020. Available at [Delayed sequence intubation (DSI) • LITFL • CCC Airway]
3. No Author. What Are The H's and T's of ACLS? American Medical Resource Institute. Available at [What Are The H's and T's of ACLS? (aclsonline.us)]